This section looks at routes of drug administration. Although many of the injecting drug users who use needle exchange do not wish to stop, some do, and promoting alternatives to injecting can be an important part of working with them.
The section also looks at the alternative methods of drug use and the pros and cons that they hold for different people using different substances.
Intravenous injection is the most prevalent injecting route amongst heroin, cocaine and amphetamine injectors. This is because:
![]() Intravenous injecting
is the quickest route for getting large amounts of the injected drug to the brain, thereby
maximising the immediate effect
Intravenous injecting
is the quickest route for getting large amounts of the injected drug to the brain, thereby
maximising the immediate effect
![]() It is associated with
less acute local infections and irritation than other routes of injection.
It is associated with
less acute local infections and irritation than other routes of injection.
It is therefore covered in detail.
Needle exchange workers should have a good understanding of all the different routes of injecting, as well as being able to promote alternatives to injecting.
Workers must know how the circulatory system works in order to be able to explain it to their clients so that they in turn have a basic understanding to help them avoid or delay some of the potential harms associated with injecting. This is therefore described first, prior to the discussion of sites and injecting technique.
How veins collapse is described in detail in Section 5: Vein and other local damage.
The
circulatory system
|
| Arteries and
veins Arteries take oxygenated blood from the lungs to the rest of the body (Figure 4.2). They progressively branch out, diminishing in size, until they reach the capillaries. The blood then passes through the capillaries in the tissues, releases its oxygen, and is collected in small veins (Figure 4.3), which by joining together progressively increase in size. The arteries return de-oxygenated blood to the lungs via the heart. Accordingly, all drugs injected into veins must follow a route back through veins of increasing size to the heart. From the heart the drugs are pumped the short distance to the lungs where the blood passes through the capillaries of the lungs to be re-oxygenated, and then they return to the heart to be pumped to the brain. When a drug is injected into a vein, it reaches the brain via the lungs in a matter of seconds. The drug is not significantly diluted: hence the experience of the 'rush' or 'hit' as the brain becomes rapidly intoxicated. The exception to this description is the pulmonary artery, which is unique because it carries de-oxygenated blood from the heart to the lungs. All other arteries carry oxygenated blood. Similarly the pulmonary vein is unique because it carries oxygenated blood from the lungs to the heart. Valves are only present in veins, and assist the flow of blood back to the heart by preventing back flow. |
Figure 4.2: Artery construction
Figure 4.3: Vein construction
Figure 4.4: Valves
|
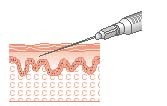
| Intravenous
injection Intravenous injecting is a highly efficient way of introducing drugs into the body. However, when drugs are injected, the filtering and delaying mechanisms that protect us when things are absorbed via the gastro-intestinal tract, lungs or skin are bypassed. The potential for infection and overdose are much increased. Figure 4.5: Diagram of an intravenous injection Correct intravenous injection technique 1. Prepare drugs for sole personal use using equipment that is only used by the injector. 2. Identify the vein to be used in some people this is straightforward, others may have to palpate (feel for) veins. Veins feel like a piece of rubber tubing under a sheet. 3. Always inject with the blood flow, i.e. towards the heart. 4. Choose the smallest possible bore and length needle for the site for superficial veins this will be a short orange or brown one. 5. Clean the site with soap and water, or an alcohol swab. 6. Introduce the needle into the vein at a shallow angle, a change in resistance is felt as the needle enters the vein. 7. Pull back the plunger to identify that the needle is in a vein a small amount of dark red venous blood should trickle into the syringe. If a tourniquet is used it should be loosened immediately after accessing the vein. 8. Inject slowly to reduce the likelihood of damage to the vein and to lower the overdose risk. Do not flush out this will significantly increase trauma to the vein. 9. Remove the needle slowly if the needle is removed too quickly, the vein may collapse. 10. Immediately apply pressure to the site bruising is caused by bleeding into the surrounding tissues. Immediate firm pressure will limit the amount of bruising caused. |
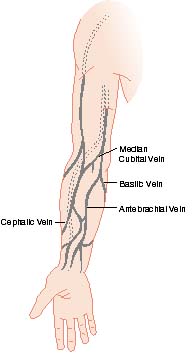
| Sites for intravenous injection
Generally, the arms are the least risky place to access veins for injecting. The main aim of advice given to injectors, after prevention of spread of blood-borne viruses, should be to maximise the length of time they are able to use the veins in their arms. When the arm veins can no longer be used, injectors should consider, and workers should promote, switching to a non-injecting route of drug use. Irreversible damage to the veins can occur where there is:
Arms The arms are the site of first choice for intravenous injecting, the superficial veins on the inside of the elbow being the most accessible. Using these sites is least likely to result in inadvertent damage to surrounding tissues and body structures, providing a good hygienic injecting technique is used. The loss of usable arm veins will leave the injector with stark choices: either to stop injecting and switch to smoking or sniffing, or to move to another site on the body with greater inherent risks. It is for this reason if no other that injectors should be encouraged to use the least damaging techniques to access veins, in the hope that this will enable them to use their arm veins until such time as they no longer want to inject, or want to stop using drugs entirely. Measures that will help to keep veins and skin healthy include:
Figure 4.6: Arm veins
|
Adapted from Getting Off Right. A Safety Manual for Injection Drug Users. Harm Reduction Coalition, New York.
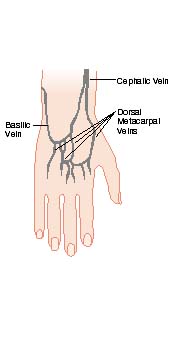
| Hands The veins on the backs of the hands can be highly visible, although they tend to be small and fragile. As it can be difficult to hide the evidence of injecting here, many avoid these sites. Furthermore, if complications such as infection or cellulitis occur, they are likely to be much more disabling in the hand than in the arm and lead to severe problems, especially if rings are left in place on the fingers. Fingers should be avoided as the veins are very small. If clients insist on injecting in their fingers, they should understand the vital importance of removing rings prior to injecting. If a finger starts to swell with a ring in place, it can quickly obstruct the blood flow leading to loss of the finger. The artery that supplies the finger lies just below the vein, if the artery is damaged the finger can 'die'. Legs The superficial leg veins are unlikely to be viable long-term prospects for injecting. They contain more valves (see Figure 4.4) which increases the likelihood of problems as injecting at or around a valve causes more turbulence and can damage the valve. The blood flow in the veins is slow, they are superficial and tend to wobble. As the flow of blood in the leg veins is upwards (i.e. towards the heart) it can be difficult to self inject in the correct direction in the legs i.e. with the needle pointing up towards the top of the leg. Because they are furthest from the heart, and due to gravity, blood flow through the leg veins is slow. If drugs are injected too fast, the veins will be unable to cope. When this happens, fluid escapes from the vein, around the needle, causing a 'miss'. The only way to avoid this is to inject as slowly as possible. Healing of injection site damage and resistance to infection are less reliable because the blood flow is slow. Abscesses and other infections are therefore a greater risk for those injecting into their legs. Varicose veins form, usually in the leg veins, because of damaged valves. The varicose vein has tight, thin walls and is often raised, stretching the skin. They should not be injected into, as they can bleed profusely. Feet Although the veins in the feet are used by some injectors, there are several factors which make them an unsuitable choice for anything other than occasional use:
As with the legs, injections in the feet should be done as slowly as possible to prevent overloading the vein. |
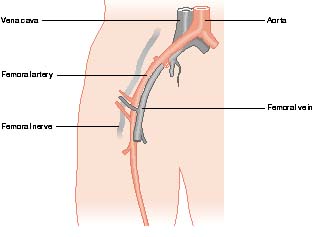
| Femoral injecting The femoral artery, vein and nerve lie very close together and their relative position varies from person to person. Grays Anatomy91, describes the femoral vein as follows: "The femoral vein accompanies the femoral artery through the upper two thirds of the thigh". (Figure 4.7) Femoral injecting is usually begun when access to the veins in the arms becomes difficult or impossible, and is always dangerous. The main dangers are:
Rozler et al. in America in 1988 noted seeing an increase in the number of complications associated with femoral injecting. As well as many of the above, these also included mycotic aneurysm and pseudoaneurysm.92 Just how dangerous and damaging femoral injecting will be on any one occasion is affected by:
|
| Figure 4.7 Representation of the relative positions of the
femoral vein, artery and nerve
This diagram should in no way be interpreted literally each individual's internal anatomy is different |
 |
| Of the dangerous sites, femoral injecting is the most frequently practised. It has to be acknowledged that some individuals with good technique use this site for many years before they experience problems. Working with femoral injectors For workers the question that should be asked is: how far should I engage or help with a potentially very dangerous behaviour, and in what ways can I reduce harm? There is a very fine line to be found between sensible information and collusion. For the worker where that line falls will depend on:
It is impossible to remove the risk from injecting into the femoral vein. It is however, possible to increase the knowledge level of many injectors about their own anatomy, without encouraging or helping with femoral injecting. By increasing the knowledge of the risk simply by using the diagrams included in this book (with the clear understanding that these diagrams are only representative and each individual's anatomy will in reality be somewhat different) some injectors may choose not to use this site. Many will not change their behaviour and choose to continue femoral injecting, sometimes requiring treatment for the results of poor injecting technique. For those agencies who prescribe injectable drugs, it would be unethical to do so to known groin injectors without confirming that their understanding of femoral injecting is sound and their technique good. An agency policy and adequate staff training on the level of advice it is acceptable to give femoral injectors will help to remove a lot of the existing uncertainty and stress for workers unfortunately, it cannot do the same for injectors. The following advice is sometimes given to groin injectors. It should be clearly understood that whilst this advice is likely to help injectors avoid accidental injection into the femoral artery, it in no way guarantees a successful injection in the femoral vein, or avoidance of the femoral nerve. It is advice that should only be given by workers who are trained and confident in their understanding of the issues, and have the support of their agency to do so. The client needs to be advised to:
This instruction should be given on the clear understanding that the worker is offering no guarantees for the safety of the procedure, which is carried out at the client's own risk. If the injector accidentally hits the femoral artery they should:
When discussing 'groin' injecting, clarification should be given that the conversation is about femoral injecting some people may think that the term refers to injecting in the penis. |
| Highly dangerous sites The highly dangerous sites included in this section such as the neck and penis are not discussed to enable workers to recommend their use to clients. It is not possible to ensure that the use of these sites is safe enough to make their promotion an ethical option. Workers may well be faced with users who are already using, or talking about using these sites. As it is often impossible to make these dangerous behaviours safe enough, workers should advocate the use of other, safer sites or routes of administration. Where the use of other, safer sites is not a possibility, workers should be heavily encouraging these injectors to:
Breasts Although there are usually small veins visible in the breasts, especially in pregnancy, it is dangerous to try and inject into them because they are very small and liable to break. They are also next to milk ducts which can be accidentally filled with fluid. Because there is no direct blood supply to the inside of the ducts, the fluid stays there and the risk of developing mastitis, infections or abscesses is high. Deep veins When searching desperately for a usable vein, some injectors will look for deep veins, by simply 'digging around'. Where this is because of a lack of awareness of available sites, supplying relevant information may be useful. For those who have limited knowledge of their body structures, education about the risks of hitting arteries, nerves or bones should be offered. Axilla (armpit) The armpit is a dangerous site for injecting because of the close proximity of arteries and nerves to the subclavian vein. Neck Self injecting in the neck is extremely dangerous, difficult to do and should be strongly discouraged. Arteries, veins, tendons and nerves are all very close together. Engaging in discussion about ways to 'make it safer' should not detract from the central message that it is too dangerous. Part of the risk arises from the fact that for self injectors, self injection in the neck requires the use of a mirror. This difficulty may lead injectors to ask others to attempt neck injection for them, thereby increasing the chances of both viral transmission and local injury, and removing all personal control over the process. It may also lay the injector open to at least a manslaughter charge if the person dies even if they requested the injection. The common complications of neck injecting may be similar to those in other areas, such as cellulitis and abscess formation93. but have even more devastating effects. An abscess or cellulitis in the neck can cause dangerous pressure on nerves or obstruct the airway. Other problems include:
Penis Injecting in the penis is sometimes attempted when other possible sites are no longer available. The penis is dangerous for injection and complications such as local infection are almost inevitable. A condition known as priapism a permanent, painful erection is a possible consequence of penis injecting. This is because an erection is caused by the veins becoming smaller and restricting the flow of blood out of the penis. For the penis to return to its normal size the veins must be able to re-open. If this is not possible because of damage, the erection will not subside. Some injectors mistakenly think that 'groin' injecting refers to injecting in the penis. When talking about groin injecting it is vital to clarify that you are referring to femoral injecting. |
| Intramuscular injection |
| Figure 4.8: Intramuscular injection | Figure 4.9: Intramuscular injection sites |
 |
 |
| Intramuscular injection is used to administer some medicines (Figure
4.8). It is not an ideal route for injection of most illicit drugs as it often leaves the
muscle stiff and sore. The exception to this is steroids which are almost invariably
injected in this way and are usually formulated for the purpose. While intramuscular injecting may be acceptable for occasional injecting, for frequently repeated doses of illicit drugs that have been acidified, it can quickly become impractical. The relatively poor blood supply to the muscle means that absorption is likely to be slow. Furthermore the fluid that has been injected can easily cause severe local infection. If injectors are injecting into muscles because they have 'run out' of superficial veins, workers need to address the issue of supporting the person in giving up injecting. Equipment and technique The equipment required for an intramuscular injection is usually:
2mL should be the maximum put into a muscle at one time. |
Subcutaneous injection
|
| Subcutaneous injection is often referred to by injectors as skin popping.
It may be done by those who are having short- or long-term difficulties in accessing
veins. It has been associated with injecting injuries since the 19th century, when it was
by far the most common route of injection. Subcutaneous injecting of illicit drugs tends to be more damaging to the surrounding skin than other routes of injection. The principle reasons for this are:
In the case of the last point, of particular concern for subcutaneous injectors is the possibility of acquiring infections such as tetanus and botulism. Although these infections are rare amongst injectors in the UK, increasing numbers of cases of both have been observed in California in the 1990s. Skin popping is more common there, and also there are suggestions that 'black tar' heroin may be sometimes contaminated by the spores of these infections.94,95 Tetanus and botulism are anaerobic bacteria (do not require the presence of oxygen) that thrive best in situations where oxygen concentrations are low, such as just under the skin surface. Tetanus is almost entirely preventable by vaccination. Skin popping is not a long-term alternative to intravenous injecting of drugs such as heroin or cocaine because of the combined effects of probable frequency of injection and irritation caused by the injected solution. One or two subcutaneous injections of street heroin will almost invariably lead to local irritation and possibly infection. Blood-borne viruses such as hepatitis and HIV can be introduced by subcutaeneous injection. |
| Figure 4.11: Subcutaneous injecting sites |  |
| Arterial injection All drug injectors should be warned that they should never inject into a blood vessel in which they can feel a pulse. Occasionally people attempt arterial injection deliberately this should be strongly discouraged. For those who hit an artery by mistake or otherwise, advice should be to:
Arterial injection can sometimes cause weakening of the artery wall (pseudoaneurysm) or fungal infection of the artery wall (mycotic aneurysm). Both conditions can lead to life-threatening arterial bleeding. Most arterial injections are accidental. Smoking or chasing heroin Smoking heroin clearly offers lower risks than injecting, both in terms of viral transmission and risk of overdose. As Southwell and Picorne say when discussing the promotion of chasing over injecting as a harm reduction strategy: "Chasing should not be viewed as a substitute for injecting, but as an alternative way of enjoying heroin. Acknowledgement should be made at the beginning that the effect does not offer the same intensity as injecting but that it does offer a gentler and less risky form of use with the added benefit of extending using episodes."96 When compared with injecting, chasing heroin will offer:
There is a potential value in using carefully thought-through campaigns promoting the smoking of heroin. It must be borne in mind that not all injectors know how to smoke it it is a difficult task requiring skill, dexterity and practice. Rectal Taking drugs into the body via the anus is occasionally practised particularly by stimulant and ecstasy users. It has been suggested by the East London and City Drug Team that drugs such as heroin might be introduced into the rectum by the anus using a syringe without a needle. If accepted by injectors it could be an alternative to injecting for some. Because of the large number of blood vessels to absorb the drug, introducing a drug into the body in this way retains some of the rush associated with intravenous drug injecting, and lowers the risks associated with sharing of equipment .97 Sniffing Sniffing drugs is usually safer than injecting them in terms of the relative danger of transmission of blood-borne viruses. Viral transmission can occur if straws etc. are used by two or more people. As with injecting, it is best for each user to have separate equipment for the sniffing of drugs. Prolonged frequent sniffing of drugs (especially cocaine) can lead to damage to the mucous membranes in the nose and cause, or exacerbate, sinus problems. Swallowing Of the commonly injected drugs, swallowing is most effective for amphetamines, which are often taken in this way, either by mixing the powder in a drink or by 'bombing' (wrapping it in a cigarette paper to reduce the unpleasant taste). If an injector is contemplating using a 'risky' substance, e.g. what is left on a spoon after filtering, swallowing usually represents the safest way of getting it into the body. For those using benzodiazepines by injection often as crushed tablets taking them by mouth is by far the safer alternative and the effect, although slower to 'come on', will ultimately be much the same. |
| Keypoints
|
©Jon Derricott
©html1999 mario lap drugtext foundation