| 59.5% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 137 |
| Yesterday: | 251 |
| This Week: | 137 |
| Last Week: | 2221 |
| This Month: | 4725 |
| Last Month: | 6796 |
| Total: | 129324 |
Section 2: The research basis for promoting safer injecting
Drug Abuse
Section 2: The research basis for promoting safer injecting
Research on the prevalence of injecting in the UK
The contribution of ethnographic research
The spread of HIV within injecting communities
The impact of needle exchange services
Promoting safer injecting practice
Opportunities to prevent initiation into injecting
Primary prevention within needle exchange
Key questions
Key points
|
There is a great deal of research evidence, from many countries, which supports the effectiveness of needle exchange programmes in helping to prevent the spread of HIV. Needle exchange appears to be most effective in combination with other interventions such as substitute prescribing and outreach programmes. Although it is impossible to evaluate the separate contributions of individual interventions, needle exchange appears to have comprehensively demonstrated its effectiveness in helping to decrease the risk particularly of HIV infection associated with injecting drug use. For workers to engage successfully with injectors, there has to be an acceptance of injecting as simply another lifestyle choice, albeit one that contains many risks. Research is now showing that avoidance of blood-borne hepatitis viruses requires more comprehensive behaviour changes than have been necessary to limit the spread of HIV. It is important that the success of syringe exchange in slowing the spread of HIV amongst injecting drug users is not allowed to breed complacency. Drug injecting and HIV infection are increasingly global issues. The number of countries reporting drug injection in 1997 was 121, and the number reporting injecting related HIV infection was 8236. Because of its illicit nature, injecting drug use tends to be hidden and difficult to quantify. It is therefore impossible to give a definitive figure of the number of injectors in the UK. The 'prevalence' also depends on the definition adopted. For example, different figures will be obtained depending upon whether prevalence is defined as people who have injected in the last:
or, in their lifetime. Several sources of information about the prevalence of injecting in the UK exist. The now discontinued Home Office Addicts Index provided national data on the number of people in treatment who injected a restricted range of drugs (including heroin and cocaine). Commonly injected drugs like amphetamine sulphate were not notifiable and the Index only identified between a fifth and a tenth of users of the notifiable drugs. In the National Sexual Attitudes and Lifestyle Survey in 1992, Johnson et al. estimated that 100000 people in England and Wales had injected in the previous five years and 175000 had injected in their lifetime38. National surveys which sample the whole population may under-report injecting prevalence because of non-disclosure of injecting and sample bias. They can nevertheless provide a useful guide to the minimum injecting population size. |
| Within individual localities, the 'capture-recapture' method has been used as an alternative way of estimating the size of the drug injecting population.
This is based on a widely used method for estimating the size of wild animal populations within a particular habitat. A sample of animals is 'captured', marked and then released. Another group is then captured and the overall population size is worked out from the percentage of the second group that is recaptured. This technique has been applied to drug injectors by 'capturing' them in two or more sets of data, for example by comparing drug agency data to police arrest data. This technique has its own limitations as the samples need to be independent, and this is rarely possible. A forthcoming publication from the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) is expected to give practical guidance for people who wish to estimate prevalence in their own localities. In order to understand how to intervene to reduce the risks from injecting, it is necessary to understand the practices that people use and the contexts in which they occur. Ethnographic research methods have been used to investigate these questions among people who inject. Ethnography was developed by anthropologists to study other cultures. Its methods are now used to study sub-cultures such as drug injecting within the developed world. Ethnography produces rich descriptions of what people do in natural settings and has proved invaluable in examining what actually happens in the injecting process. Ethnographic research is useful when examining areas of behaviour about which little is known. The findings are often later used to develop questions in larger scale surveys. As Lambert and Wiebel have said: "It is at this exploratory stage of research that ethnographic and qualitative methods can make significant contributions to the knowledge and understanding of problems and to the formulation of subsequent questions for quantitative research."39 Many fundamental understandings of injecting behaviour, such as the identification of frontloading and backloading, have been identified through ethnographic research (see page 48). The similarities between ethnographic methods and aspects of outreach work have been noted. This has led to its incorporation within some outreach work and the development of models of practice that integrate ethnography and outreach40,41. |
|
In a comprehensive and succinct review, Bloor42 has summarised the spread of HIV among injectors internationally. Key points include:
Preconditions for rapid HIV spread Gerry Stimson43 has identified three conditions necessary to produce an HIV epidemic amongst injecting drug users: 1 A substantial population of injectors 2 The potential for HIV transmission i.e. equipment sharing as a cultural norm 3 The presence of HIV. These preconditions are present in locations all over the world. In many countries where there were few if any measures such as needle exchange to help prevent the spread of HIV, it has spread extremely rapidly amongst injecting drug users. Table 2.1 gives a clear indication of what can happen when harm reduction measures are not in place. This pattern has been, and continues to be, replicated in many countries across the world. |
|
| Table 2.1: Prevalence of HIV and restricted availability of sterile injecting equipment | |
| Place Early % of IDUs Time span % of IDUs tested HIV
tested HIV positive (years) positive after time New York City 10 5 50 Edinburgh 0 1 40+ Bangkok 2 1 40 Manipur (India) 0 1 50 (Adapted from Des Jarlais et al.44) |
|
International findings In a review of studies conducted in five cities that all had a low baseline of HIV positive injecting drug users, and implemented large-scale availability of sterile injecting equipment, Des Jarlais et al.44 observed that the high rates of HIV seroconversion (see Table 2.1) do not occur. Under these circumstances, prevalence can be stabilised or decrease, as shown in Table 2.2. Table 2.2: Prevalence of HIV and wide availability of sterile injecting equipment Place Early % of IDUs Time span % of IDUs tested HIV tested HIV positive (years) positive after time Glasgow 4 6 1 Lund (Sweden) less than 2 6 less than 2 Sydney 4 7 4 Tacoma (USA) 0.4 5 3 Toronto 0 5 2 (Adapted from Des Jarlais et al.44) Studies showing rising HIV seroprevalence, after the introduction of needle exchange In Vancouver and Montreal high levels of HIV have developed among injecting drug users in spite of established needle exchanges in both cities. Strathdee et al.45 suggest that in Vancouver this may be because:
This Canadian evidence is unusual and has been seized on by critics of needle exchange. Rather than showing that needle exchange is ineffective, it may best be taken as a reminder that needle exchange alone is not necessarily enough. Aspects of the way the service is provided, and the availability of complementary services, such as methadone maintenance, can make it more (or less) effective. |
| UK HIV prevalence rates
In terms of the three preconditions for an HIV epidemic identified by Gerry Stimson, in 1984, the UK had:
This being the case the continuing low prevalence of HIV among injectors during the 1990s represents a significant success for harm reduction interventions. However, as the preconditions for an epidemic still exist we cannot be complacent. As Stimson has said: "the HIV epidemic has been averted, not prevented."35 The consistent prevalence rate of HIV amongst injecting drug users tested by the Public Health Laboratory Service in England and Wales (excluding London) is about 1%46. The prevalence rate in London is thought to be about 7% or less47. In Scotland the prevalence of HIV infection in Edinburgh in the mid-1980s of 50% or more amongst injectors tested, is now running at around 20%. In Glasgow, the rate is similar to England and Wales at around 1%. The total number of AIDs cases related to injecting drug use in the UK to the end of 1997 is 94548. The cumulative number of HIV cases between 1985 and 1997 attributed to injecting drug use is 3147 out of a total of 31001, or about 10% of cases. The incidence of new HIV infections is low, about 130 cases per year in England and Wales, with about 75% of these cases being in London.48 The pattern of the English HIV epidemic Epidemiologists have shown that the peak and subsequent decline of incidence of HIV infection amongst injecting drug users in London occurred between 1983 and 1986 (Figure 2.1). HIV cases attributed to IDU Figure 2.1: Estimated annual HIV incidence from IDU. Adapted from A Sexual Health Ready Reckoner49 |
|
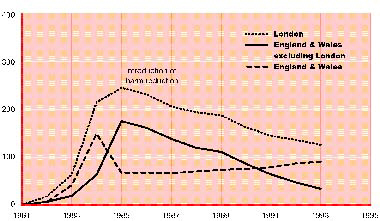 |
| Interventions such as needle exchange came into being slightly after the peak, which suggests that whilst needle exchange and associated interventions are very likely to have assisted in the decline in incidence of HIV amongst injectors, other factors may be involved.
These other factors are likely to have included behaviour changes triggered by HIV public information campaigns and reinforced by the introduction of formal needle exchange facilities. Harm caused by needle exchange Some concerns about risks from the introduction of needle exchange have been voiced. These include:
A report prepared for The Lindesmith Centre in 1997 cites six previous reports prepared for the American government, that all concluded that access to sterile injecting equipment does not increase injecting. They also noted that in American needle exchange programmes the minimum age of injectors had remained stable, while in Amsterdam, the average age of injectors is increasing50. It is possible that the absence of widespread availability of sterile injecting equipment might lead some injectors to decrease or abandon injecting as a preferred route. When imprisoned, some injectors stop injecting. Regrettably, others move towards higher risk forms of injecting, resulting in outbreaks of HIV and hepatitis B infection51. Furthermore, evidence from around the world suggests that in times of needle and syringe scarcity, many injectors simply adopt riskier practices that involve sharing more often, and with more people such as in shooting galleries.
The promotion of safer injecting practice forms a cornerstone of needle exchange policy and community interventions. Formal needle exchange, and community interventions should consist of much more than the basic requirement of providing appropriate clean equipment to injectors. Raising the topic of safer injecting and providing appropriate understandable information to clients and into injecting networks is an essential part of the process. Evidence for behaviour change A 1988 study by Power et al. examined a group of 127 regular drug users between 1986 and 1987; 115 of whom had injected at some time in their life. Of this 115, 12% ceased injecting during the time of the study around 65% of these said this was because of concerns about AIDS. Forty-two percent of the 115 were still injecting but said they were no longer sharing, although less than half of these said this was because of concerns about AIDS. Reasons given by those who were no longer sharing, but not because of concerns about AIDS, includes easy availability of equipment and concerns about hepatitis52. Before the widespread introduction of needle exchange, the level of equipment sharing was relatively high. Sharing has reduced but persists, particularly among sexual partners and close friends (see Section 3: Viral transmission, drugs and their preparation). There are now many reports53,54 of injecting behaviour change, including changes in the:
|
| Des Jarlais et al. reviewed studies on syringe exchange attenders in the five cities described in Table 2.2. This showed that between 73% and 87% of those interviewed in the different sites had changed their behaviour in some way because of concerns about AIDS.44
Injecting and risk Injecting drug use is by far the most hazardous way of introducing drugs into the body. A large body of research shows that it creates a risk to health from:
It is obvious to suggest that the best way of reducing the harm associated with injecting will always be to stop injecting. However, it is now well established that many injectors do not want to stop and also do not want to be offered 'treatment' for their injecting. It is evident that needle exchange is an effective way to reduce the sharing of needles and syringes. Particularly in light of our current understanding of the hepatitis C epidemic, there is a need for further development and evaluation of interventions which are focused on reducing the risks from injecting. Increasing the effectiveness of needle exchange It is widely believed that the effectiveness of needle exchange is increased because of the opportunities it offers for one-to-one, brief interventions with people who inject. These represent the 'added value' of specialist syringe exchange over other forms of provision such as pharmacy exchange. There has however been little published work on this aspect of needle exchange. Interventions may focus on information and awareness of unconsidered risks such as 'backloading' or needlestick injuries. They may involve the development of skills to manage particularly persistent and difficult situations such as sharing between sexual partners. They can give guidance on the prevention and management of overdose and can also involve the provision of low-threshold access to a range of other primary care services such as viral testing, sexual health promotion, hepatitis B vaccination or general health checks. Needle exchange provides valuable contact with a socially excluded group. Further research is needed into the true extent of the largely unrecognised 'added value' of the work that is conducted and the ways that it can be further increased. Making appropriate contact For needle exchanges to be effective, they have to make and maintain contact. Successful projects have achieved this by being easily accessible, welcoming and by treating drug users with respect. There have been examples of unsuccessful projects, which may have failed to make contact with many injectors because of a combination of:
|
| The effect of different intervention strategies
There has been considerable attention paid to researching the extent and nature of risk behaviours among people using syringe exchange and those who are 'out of contact'. By contrast, there has been less focus on the detailed practice of syringe exchange work such as:
Some information giving is generally presumed to accompany the dispensing of clean equipment. This process has however received comparatively little attention. Work by Speed and Bennett55 in 1997 suggests that it may be a mistake to presume that some of these basic activities occur in the way that is commonly supposed. Variations in the context, philosophy and organisation of specialist services mean that specialist syringe exchange work is conducted in different ways. The lack of systematic study of the communications and intervention strategies, or the scope of work, means that we have relatively little understanding about how these variations affect outcomes, or even the range of strategies used. Especially in the light of concerns about HCV, there is an evident need within syringe exchange services to evaluate the effectiveness of different approaches to the achievement and maintenance of health behaviour change related to injecting risk. In doing so, it would seem useful to follow Pawson and Tilley's56 approach to evaluation. This examines the influence of both 'contexts' and 'mechanisms'. 'Contexts' influencing syringe exchange Factors involved in the context of a service include whether the service setting is:
Other factors include the level of:
And whether the service is:
In addition to the above, an important factor is the operating philosophy of the service which could include:
'Mechanisms' used to promote change The mechanisms deployed to achieve change include:
If systematic risk assessments are conducted, are they assessing risk of:
Other mechanisms include:
|
| Targeted interventions and campaigns can either be aimed at specific risk behaviours, for example:
or at specific populations, for example:
Syringe exchange was originally developed to perform a secondary prevention role, namely, avoiding the acquisition of HIV infection among people who have begun injecting. This remains its key objective. However, it is increasingly clear that:
non-injectors as part of syringe exchange. The intervention is based on the following insights from research:
The intervention had five main objectives:
The intervention was brief and consisted of:
The outcomes of Hunt's study were encouraging: the intervention was successfully delivered and was acceptable to both injectors and drug workers, and at a three-month follow-up in a sample of 73 people:
|
|
Syringe exchange is a successful example of secondary prevention. When people have begun injecting, syringe exchange acts to prevent potential harm. There are however, opportunities for primary prevention as part of syringe exchange, as have just been described. Such interventions would give added value to syringe exchange in a way that will be increasingly sought by purchasers. With the growing calls for ways of preventing injecting, this type of intervention offers part of a possible solution. By adopting such work and seeking similar opportunities, it is possible to achieve an important public policy objective, and also put specialised harm reduction services on a more secure footing by adding to the value of the service. It is important to clarify that such work is not an argument for prevention evangelising within syringe exchange. It is essential that the accepting, non-judgemental ethos of syringe exchange, which underpins its success, is not jeopardised. If someone chooses to inject, a syringe exchange is definitely not the place where they should feel admonished or overly pressurised to stop. Nevertheless, injectors will sometimes choose not to inject someone else, choose not to promote injecting, or choose to use other routes of administration. Supporting people in these choices seems a practical and legitimate activity within syringe exchange services which may have an important preventative function as well as buttressing the position of harm reduction services. Audit involves measuring the performance of services against a standard. It could be a valuable tool for measuring the effectiveness of particular aspects of needle exchange schemes. The absence of any comprehensive audit tool for needle exchange has hindered the development of services. In a rare exception to this, an audit of risk behaviours amongst injecting drug users attending syringe exchanges in North West England took place in six exchanges in 199755. The great majority of the 96 injecting drug users interviewed were primarily heroin injectors for whom injecting was their primary or only route of use. This audit found that sharing of paraphernalia (spoons, water and filters) was extensive. Over 50% of the sample said that they had never received information about the risks of sharing paraphernalia. Only 4.2% said they had received information about risks associated with paraphernalia from a drug worker. Spoons were the item most frequently used at the same time or after someone else. Worryingly, over half of those interviewed said that they did not know of any risks associated with these practices. About 33% mentioned the potential risks of HIV, hepatitis or both. In contrast, a low number (8.2%) of the subjects reported using a syringe and needle after another person. |
| The recommendations of the audit were that drug service commissioners should:
Drug service managers should:
Drug workers should:
|
|
Wodak58 has identified several key unanswered questions that must be addressed in order to prevent the continued global rise of HIV infection amongst injecting drug users:
In countries such as the UK, where injecting equipment and harm reduction services are available, the key question for the future is probably how can the spread of hepatitis B and C through the sharing of injecting paraphernalia be prevented? |
![]() A considerable body of evidence shows that the health behaviour of people who inject can change when they are aware of the risks from shared needles and syringes and have access to clean injecting equipment.
A considerable body of evidence shows that the health behaviour of people who inject can change when they are aware of the risks from shared needles and syringes and have access to clean injecting equipment.
![]() The effectiveness of syringe exchange and related harm reduction policies has almost certainly been crucial in keeping HIV prevalence rates among injectors in the UK as low as they are.
The effectiveness of syringe exchange and related harm reduction policies has almost certainly been crucial in keeping HIV prevalence rates among injectors in the UK as low as they are.
![]() In countries where effective harm reduction strategies are not implemented, HIV prevalence rates amongst injectors can rise to over 50% in only a few years.
In countries where effective harm reduction strategies are not implemented, HIV prevalence rates amongst injectors can rise to over 50% in only a few years.
![]() There has been relatively little research conducted into how workers interact with clients and the effectiveness of different approaches. Further work is needed to develop a better understanding of what constitutes 'best practice'.
There has been relatively little research conducted into how workers interact with clients and the effectiveness of different approaches. Further work is needed to develop a better understanding of what constitutes 'best practice'.
![]() Research into an intervention to prevent the initiation of new injectors suggests that significant primary prevention gains can also be achieved within needle exchange services. Further development of this aspect of syringe work is necessary.
Research into an intervention to prevent the initiation of new injectors suggests that significant primary prevention gains can also be achieved within needle exchange services. Further development of this aspect of syringe work is necessary.
![]() Audit is an important means of promoting and encouraging effective interventions. There is a need to develop a comprehensive audit tool for needle exchange and increase the way that audit is used to improve services.
Audit is an important means of promoting and encouraging effective interventions. There is a need to develop a comprehensive audit tool for needle exchange and increase the way that audit is used to improve services.
Last Updated (Wednesday, 05 January 2011 23:37)