| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 161 |
| Yesterday: | 251 |
| This Week: | 161 |
| Last Week: | 2221 |
| This Month: | 4749 |
| Last Month: | 6796 |
| Total: | 129348 |
| - |
Drug Abuse
C.4 PATTERNS OF USE
In discussing the process whereby persons become introduced to and involved in, and depart from the use of drugs, it is helpful to employ the concept of a 'social career' as delineated by Becker and others.15, 96, 268, 278 The notion of 'career' permits the understanding of behaviour patterns as developing in an orderly sequence that any individual may pass through—for example: 'experimental', 'occasional', and 'regular' drug user. Attainment of each step in the sequence is a necessary condition for further career advancement, although this developmental process may be terminated or reversed—with varying difficulty, depending on the drug—at any stage.
The concept of a drug career, however, does not necessarily imply that a particular variety of drug use assumes a predominant or determining role in an individual's life. In some cases, of course, this actually occurs—heroin, methamphetamine ( `speed') and alcohol dependence being the archetypal examples of this development. In most instances, however, a person's drug-using career is subordinate to other aspects of his life (his academic, occupational and familial careers, for example) and patterned by these conventional demands and obligations. A drug-using career, then, is simply a natural history of drug use: that orderly sequence of stages through which any individual may progress between initial and chronic use of a drug.
It is possible to describe individual career routes for every psychotropic drug. This approach, however, would tend to hinder appreciation of the fact that the process of drug use socialization is basically the same no matter which drug or drug-type is considered. For this reason, the following discussion applies generally to all drugs. There are, however, junctures at which it is critically important to distinguish specific drugs and drug careers from this general framework. In such instances, the differentiating properties will be
discussed and, when necessary, particular career patterns associated with specific drugs or drug combinations will be more comprehensively developed.
Drug use—like any social, recreational or vocational activity—is learned behaviour.* Consequently, the process of becoming a drug user is essentially identical to the learning of behavioural patterns within any sociocultural context. In the case of drugs, a novice must first learn to accept the idea of his personal use of drugs. Subsequent use is likely to depend on learning to acquire, prepare and administer drugs, learning to subjectively appreciate their effects, and learning to accept their use as appropriate behaviour under certain circumstances. The regular use of a drug requires learning the role of `drug user' and, in some cases, learning to become a member of a drug-using subculture. The discontinuation of, abstinence from and relapse to the use of drugs also involve learned behaviours. Learning, then, includes many aspects of drug use: ingestion, patterns of use (frequency, drug preferences, social contexts), meanings of the drug experience, ideology and values, and a host of esoteric skills related to the procurement of drugs and, in some instances, the maintenance of a drug dependence.
This socialization process can best be described with reference to a typology of drug users based on levels-of-drug-use (see C.1 Introduction above). These level-of-use distinctions—initial or experimental use, occasional use, and regular use—can be viewed as three identifiable gradations on a continuum of increasing personal involvement with drugs and drug-related activities. These level-of-use categories can also be conceived of as three stages of socialization into drug use, albeit with the caution that progression to any advanced stage is neither irreversible nor a necessary or inevitable consequence of entry into a preceding stage.
INITIAL OR EXPERIMENTAL USE
`Experimental' users of a drug are those persons who have not yet learned to effectively use and positively interpret the effects of the drug in question. They usually have no regular access to supplies of the substance, and they are unlikely to have assumed the definitions and evaluations of the using culture. Persons who try a drug but never learn to recognize or appreciate its psychotropic effects are unlikely to advance to occasional use of the drug. They will, instead, terminate their use after a few experimental sessions.
As was pointed out in the Cannabis Report with respect to marijuana and hashish, the initial use of a drug almost always depends on a willingness to try that drug.* The exact motivating factors—whether psychological or sociocultural—that predispose an individual to drug use may vary from drug to drug and from individual to individual (see Appendix D Motivation and Other Factors Related to Non-Medical Drug Use). However, the willingness to initially experiment (whatever its etiological source) depends on the potential user's interpersonal and attitudinal situation (discussed on the following page) and his effectively dealing with three major social control mechanisms: limited availability, the need for secrecy, and the relative immortality of the act as publicly defined.'3. 14 Advancement through the stages of a drug-using career will only occur once any inhibiting effect of these controls has been successfully neutralized.
It is important to recognize, however, that the valence or strength of these controls varies from drug to drug, from reference group to reference group, and from time to time. Alcohol and tobacco products, for example, are much more readily available than are the illicit drugs—although access to these substances is still restricted by legal regulations and more informal familial rules that primarily affect use by children and adolescents. Similarly, the need for secrecy resulting from the fear of disapproval or other negative sanctions does not usually apply for most adult use of licit psychotropic substances, but would have some inhibiting effect on most illicit drug experimenters and those adults who dwell in communities which express and follow temperance values. It should be noted, as well, that conventional definitions of appropriate drug-using situations compel many adult users of licit drugs to be secretive about their consumption; for example, a business executive anticipating a tense conference may imbibe alcohol in the privacy of his office in order to keep his co-workers from learning of his indulgence and commenting unfavourably. The non-medical use of 'pep pills' by housewives, athletes and businessmen may also be hidden from friends and relatives for similar reasons.
Public definitions of various types of drug use also change over time and, consequently, alter the moral context of such use and the inhibiting force of these moral considerations. Cannabis use, for example, has recently been divested of many of its negative moral connotations, while the non-medical use of amphetamines has suffered increasing stigmatization over the past few years. Despite these variations, it appears that initial drug use depends on the neutralization of these three social controls—although some types of experimental use are more easily arranged and justified than others.
The problems of availability, secrecy and stigma are usually resolved within the context of initial drug use. Obviously an individual's willingness to try a specific drug is at least partially a function of his previous drug experiences, if any,* and some degree of anticipatory socialization that predefines the event as relatively attractive or unattractive. Once one is open to a drug experience, however, his actual use of the drug is more likely to occur in an aleatory—although natural—rather than deliberate fashion. Furthermore, one's initial experience with a specific drug—regardless of the drug or previous drug experiences—is likely to transpire in a social situation in which such behaviour is both tolerated and typical. As Sadava has noted: "The crucial point to be made here is that drug-using behavior . . . is not [usually] a sudden dramatic change in the individual's life and values, but develops as a natural, i.e., not surprising, process within the sociocultural context."229
Alcohol use, for example, is likely to begin in early or mid-adolescence, with parental permission being granted to test small amounts of the drug in the household living or dining room. Alternatively, a teen-ager may be introduced to alcohol by his peers at a party or after school. In either case, the problems of availability, secrecy, and stigma are resolved by influential friends or relatives who sanction the activity, furnish the drug, and provide a setting relatively safe from legal intervention. The initial use of other drugs occurs in a similar manner, except that parental influence is often replaced by the influence of trusted drug-using friends, relatives or a single intimate (such as a spouse or lover) in the case of illicit substances.
The naturalness of this initiation process is clearly evident in the case of heroin—the most stigmatized and one of the least accessible of all currently used drugs. Many researchers report that a close, friendly association with heroin users almost invariably precedes first use of the drug.36, 57, 73, 121, 147, 150, 253, 268 Initial use, when it does occur, is usually (but not always) a spontaneous and unanticipated event in which the experimenter is often gratuitously provided with an opportunity to try the drug.57, 117. 121, 150 The novice's initiators are most often experimental or occasional users themselves who—by virtue of their non-dependent state—claim to be in control of their heroin use.]' Thus, the initiators mitigate the new user's anxieties about the potential dangers of heroin use by presenting themselves as 'living proof' that dependence does not necessarily follow even extensive experimentation.268 Furthermore, the drug is sincerely offered to non-users as a pleasant experience rather than out of any desire to cause harm or injury. As Hughes and Crawford, in a recent study of heroin initiation and diffusion in Chicago, have observed:
... initiation to heroin usually occurs in a small group setting, involving only the new user and one or two addicts or experimenters. Most frequently, the initiate is introduced to heroin when he meets a friend who is on his way to cop [purchase] or is preparing to "fix" [inject]; he rarely seeks out the drug the first time. Thus, initiation depends more on fortuitous circumstances than on a willful act by the new user."'
It should be noted, however, that—theoretically—the first use of a drug need not derive from social interaction with users of that drug. Initial use may also occur as a consequence of accidental discovery of a substance's psycho-tropic effects (as occasionally occurs with the volatile solvents) or as a result of exposure to media presentations or hearsay which leads to a deliberate decision to obtain and try the drug. However, except for certain licit drugs (such as most solvents, some hallucinogens such as nutmeg, alcohol, tobacco, and pharmaceutical preparations such as amphetamines and sedatives which may be removed from family medicine cabinets) and certain privileged populations (such as the medical profession), the problem of availability remains and, consequently, almost all initial drug use results from interpersonal introductions to the drug. The Commission's university survey, for example, found that only three per cent of Canadian college cannabis users had first tried marijuana or hashish by themselves.'"
The one major exception to the social and fortuitous nature of this initiation process involves those persons who purposefully and privately employ drugs for self-medication or improved functioning. Members of the medical profession—who are familiar with the medical properties of drugs and who have constant access to them—constitute the best documented example of this practice. Whereas illicit drug users generally experience initiation in a primary group setting, doctors and nurses almost always first ingest or inject their drugs in isolation and attempt to maintain the secrecy of their use. By way of illustration, Winick found that not one of his sample of 98 ,physician-addicts had been introduced to opiate use by others, and that 25 per cent of the doctors' wives were unaware of their husbands' dependence.277 It appears, then, that in the case of doctors, professional training and occupational access to drugs substitute for the interpersonal socialization that characterizes most types of drug initiation.
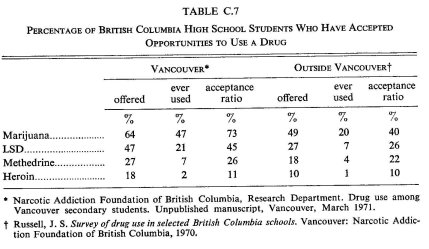
While availability is obviously a crucial factor in initial drug use, it is clear that only a fraction of those persons granted an opportunity to try a drug actually do so. Goode has reported that 46 per cent of his sample of 200 marijuana users had declined opportunities to try marijuana prior to their initial use," and a Commission survey of Canadian adults found that only 25 per cent of those respondents who had been offered LSD had in fact used this drug. 142 Furthermore, it appears that the proportion of those who accept an offer to try a drug is inversely related to the perceived danger or stigma of that drug: the greater the perceived danger or stigma, the lower the proportion of users among those who have access. Table C.7 illustrates this relationship for two British Columbia high school populations.
Goode has suggested that the decision to experiment with a new drug is dependent on the novice's perception of the relative danger involved in such use, his perception of the drug's benefits, his attitude toward users of the drug, and his closeness to both the drug's endorsers and those who have proposed the.initiation.99 Several investigators have reported that the most important determinant in regard to initial experimentation is the degree of `trust' that an initiate feels for those offering him an illicit drug.48• 59, 63, 230
In some cases, a particular mode of administration may have as great —or even greater—an inhibiting effect on initial use of a drug as the novelty of the drug itself. Previous drug experiences play an important role in this regard: users of tobacco products are unlikely to balk at the prospect of having to smoke marijuana, hashish or opium, and the swallowing of a pill, capsule or tablet (as is the ordinary mode of ingestion in the case of hallucinogen and sedative use) is such a universal procedure that few, if any, novices would hesitate to use a drug because of this administration technique. However, other modes of administration—such as the 'snorting' (nasal inhalation) of cocaine or the use of plastic bags with certain volatile solvents—may be sufficiently alien to many persons to at least intially deter them from such experimentation.
The most dramatic illustration of the inhibiting force of administration techniques concerns the use of drugs that are usually used parenterally (i.e., by injection) such as heroin and 'speed' (meth amphetamine). These substances may be snorted rather than injected, but an initiation opportunity is most likely to occur in a setting in which experienced users are intravenously using the drug. Parenteral techniques (be they subcutaneous, intramuscular, or intravenous) are generally considered painful and, as such, are anathema to most persons whose modes of drug administration, if any, ordinarily consist of swallowing or smoking. For those individuals who have previously injected drugs (usually hallucinogens), the transition to intravenous use of speed or heroin is not difficult. But, for most, this style of use represents a critical departure from their normal drug consumption patterns. One Montreal speeder clearly expressed the significance of such usage:
When you start using a syringe that indicates that you're using heavy drugs—that you're really into the drug scene. The syringe is the cutting off point between soft and heavy drugs."'
Despite these apprehensions, most persons who have an opportunity to try speed or heroin and have decided to do so will allow an experienced user to inject them once their fears have been verbally or demonstrably allayed.
It is reasonable to assume that someone interested in initially trying an illegal drug will usually take either the first one which is offered to him by trusted friends or that drug which he considers the least dangerous of those available to him in his social milieu In many cases, cannabis is the first illegal psychoactive drug to which an individual will have access, but the use of one or more of a wide range of other drugs usually predates marijuana or hashish use. Various studies have shown that the use of prescription drugs, barbiturates and amphetamines, glue and other volatile solvents, tobacco and alcohol often precede the use of cannabis.
When questioned about their early drug history, the majority of nonmedical users reveal that their first experience was with alcohol. In the mid-fifties, Stevenson and his associates found that almost all of the British Columbia heroin users they studied had used alcohol prior to opiates and most of them had never tried cannabis.263 As noted earlier, it was not until the mid-sixties, when cannabis became readily available in western Canada, that heroin users indicated concurrent or prior use of marijuana.127 Alcohol, as the first drug used by heroin addicts, has been reported by Henderson, Chambers, Robins, Darvish and Murphy, and Kosviner, et al.52' 117, 137'215 Hawks and his associates discovered that problem drinking predated the use of other drugs among amphetamine users;113 Whitehead found that alcohol and tobacco use generally precede solvent use;274 and cannabis-using college students studied by Goode had first used alcohol.99 Moreover, two extensive surveys; one of a college population238 and the other of high schools," found that alcohol-using students were much more likely to want to try marijuana than were non-drinkers.
Heroin users have often consumed a wide variety of other drugs prior to opiate use.268 In Vancouver, Johnston and Williams found that in one sample of 186 heroin users, 11 per cent had first used amphetamines, 20 per cent first used hallucinogens, and 32 per cent first used barbiturates, while the remainder (37 per cent) had used cannabis first.127 These respondents, however, were not questioned about their use of alcohol or tobacco. It is evident that for almost all adolescents, the first psychotropic drug used is either alcohol or tobacco."° Unfortunately, many investigators do not ask about these drugs when collecting drug-use histories of their subjects. Although tobacco and alcohol are legally distributed, the first use of these drugs is often by children or adolescents who are under the minimum legal age.
The use of a number of other legal substances may also predate illegal drug use. A number of studies have discovered that the non-medical use of codeine cough syrups has preceded the use of illicit substances.14°. 166 Barbiturate use has often been found to precede the use of other 'dangerous drugs' and heroin.103, 282 Glue and solvent sniffing may often occur before the use of cannabis or other legally prohibited substances. The relationships among various patterns of non-medical drug use are further discussed in C.4 Patterns of Use, "Patterns of Multiple Drug Use".
OCCASIONAL USE
In the Cannabis Report occasional users were defined as those persons who consume marijuana or hashish once a month or less. Such operational definitions, however, are inappropriate to a discussion of patterns of drug use in general, as level-of-use distinctions based on frequency and regularity of use are a function of the effects of the drugs being considered, their relative availability, and their legal status. For our purposes then, occasional use will be understood as that using pattern characterized by episodic consumption dependent on fortuitous developments such as the sharing of another's drug in a social setting. Occasional users do not usually maintain a personal drug supply and the use of psychotropic substances has only a marginal role in these persons' lives. Generally speaking, the occasional use of drugs represents a recreational diversion that is approached with a 'take it or leave it' attitude.
The occasional consumption of a drug is usually the first stage of continued drug use beyond initial or experimental use and, as such, is dependent on learning to effectively use and positively interpret the effects of the drug. There are several learning processes which are generally considered prerequisites to any continued use of a psychotropic substance. These include mastering the modes of administration necessary to achieve a desired drug effect, learning to perceive these effects as drug induced,* and learning to subjectively interpret these effects as pleasurable or functional and, therefore, worth at least occasional repetition. These 'lessons' usually result from participation with more experienced users who educate the novice as to the most effective means of consuming a particular drug and sensitize him to those psychological effects which they value and which positively reinforce their continued use. This social education of an occasional user is also likely to include information about safe dosage levels, appropriate behaviour, legal precautions (if necessary), and those activities which are felt to be enhanced by use of a particular drug.
Apart from the desire to be stylish or to avoid embarrassing oneself or one's host, any continued use of a drug—be it occasional or more regular —depends, at least, on the internalization of these first lessons: learning to correctly use a drug, and learning to recognize and appreciate its effects. In the case of some drugs, however, an occasional—rather than regular—consumption pattern may reflect limited availability, prohibitive costs or fear of legal intervention, rather than the 'take it or leave it' attitude that ordinarily characterizes this level-of-use. Cocaine, for example, is often reported as a favourite drug by persons whose financial situation or range of drug-using acquaintances restricts their use to those infrequent occasions when they are fortunate enough to come into contact with persons who possess the drug. In cases such as this, the drug is strongly desired and a regular pattern of use is only avoided because of situational rather than motivational factors.
Finally, it should be noted that the occasional use of a drug may follow as well as precede a period of regular use. This possibility is discussed below in the context of termination and reduction of regular drug-using patterns.
REGULAR USE
Although many individuals remain on a level of drug use that is occasional, spontaneous and serendipitous, for others use becomes a regularized pattern governed by normative restraints. Alcohol is a case in point. For some, it is only used in exceptional circumstances; for others, alcoholic beverages will become a natural adjunct to certain activities or will be consumed on specific occasions in a regular fashion, before dinner or while watching sporting events on television, for example. This does not mean that alcohol will always be a part of these situations, but there is a higher likelihood that it will be used then than at other times.
Not all drugs are used regularly in the same way. Coffee, tea or tobacco are usually consumed throughout the day. Similar patterns of alcohol use are less common and generally restricted to those who are considered in North American society to have a 'drinking problem'. However, regular or ritualized daily use of moderate quantities of alcohol (taking wine with meals, for example) is not considered by most people to be an incontinent level-of-use. With regard to illicit drugs, recent studies of regular cannabis users tend to suggest that patterns of use of marijuana or hashish are somewhat similar to those of alcohol, and that for some users these substances are essentially social or functional equivalents.'87 Frequent use of LSD or cocaine, on the other hand, is a comparatively rare phenomenon for reasons specific to the effects or the availability of these drugs.
The usual levels of regular use that are attained by non-medical drug users vary according to the kinds of substances that are consumed. In the Cannabis Report we operationally defined 'heavy-regular use' as smoking cannabis from twice per week to several times per day. For this substance this is a reasonable definition that would be accepted by most researchers as well as a proportion of users themselves. However, for a substance such as tobacco, even two or three times per week or one cigarette per day would be considered a moderate to light level-of-use compared to the use levels of most tobacco smokers. Similarly, 'moderate-regular use', as we have earlier defined it, may involve the ingestion of cannabis several times per week. This would probably be a reasonable and meaningful operational definition of moderate-regular alcohol use, as long as the doses were not excessive, but would represent a heavy use pattern for a drug such as LSD. Thus, each drug requires its own operational definitions of what constitutes 'light-% 'moderate= or `heavy-' regular use.
Some regular drug use patterns involve daily or even hourly administration; others entail less frequent use, but are nonetheless 'regular' insofar as the drug is usually taken in specific situations or under certain conditions. For our purposes, 'regular use' is any pattern of drug use that involves systematic consumption of a drug, even if the frequency of use is quite low. Regular drug use assumes that the individual has developed a set of norms or rules governing the appropriate times and places for drug use as well as the usual dosage levels. In many cases, official and unofficial rules not only regulate drug-taking behaviour, but also behaviour while under the influence of these substances. In the light of this definition, ceremonial or ritual use of drugs (such as alcohol and peyote) is one type of regular use pattern, even though it may only occur once or twice per year. Thus regular use may involve heavy or high-dose use, but these use levels are not necessary conditions of regular use patterns as we have defined them.
BECOMING A REGULAR USER
There are a number of factors which affect the likelihood of establishing a regular use pattern, the dosages likely to be consumed and the frequency and situations of drug administration. In the following section we will deal with those variables which govern the ease or difficulty of adopting behavioural norms of regular non-medical drug use.
THE LEGAL FRAMEWORK
Although alcohol is one of the most popular drugs in non-medical use in Canada, local laws and statutes restrict the times during which it can be purchased (in some 'dry' counties, banning purchase altogether) and the situations in which the beverage may be consumed. There are also restrictions on the age of the users. Some of these restrictions are circumvented, disobeyed or rarely enforced (the public consumption of alcohol at sporting events, for example), but they still act as constraints on the drinking behaviour of most people. In addition to regulations governing when and where alcohol may be drunk, there are also restrictions on what activities an individual may participate in while under the influence of alcohol, from operating a motor vehicle to being 'drunk and disorderly' in a public place. The purchase of tobacco products is restricted to those over a certain age limit, but otherwise there are few legal restraints on its use other than forbidding smoking in certain theatres, public buildings or conveyances. Coffee, tea, and over-the-counter preparations are universally available and governed only by controls on their manufacture, advertisement and wholesale distribution. There are literally thousands of products on the shelves of retail stores which contain solvents or propellants which may be used for their psychotropic effects. They remain readily available for socially approved purposes, thus making legal control of their use for intoxication extremely difficult. Illicit drugs are much less readily available to most users.
AVAILABILITY OF DRUGS
In order to establish a regular drug use pattern, it is necessary to obtain a sufficient and relatively continuous source of supply. For some users, this source will necessarily be illegal or quasi-legal. Adolescents who have not yet attained the legal drinking age or are too young to purchase tobacco must rely on adults or older adolescents to obtain these drugs for them unless they appear to be older than their years or have been able to obtain forged or stolen identification certificates or those of older friends. For many substances, there is no legal source for the non-medical drug user.
Becker proposed that obtaining a regular source of supply of cannabis was one of the most important aspects of becoming a regular marijuana user." The necessity of establishing a source of supply is an important factor in becoming a regular user of all illicit drugs, although some substances are more readily available than others. Over the past few years, many drugs which were once difficult to procure have become readily available from a wide variety of sources.
Most non-medical drug users are introduced to the use of their drugs by friends or acquaintances and these friends are also likely to serve as sources of access to the illicit market. In some cases the first regular contact with an illicit marketplace will occur when a group of friends pool their purchasing resources, thus reducing the unit price of the quantity each uses for personal consumption.99 Cannabis and LSD users are particularly likely to purchase a specific amount for use over a period of weeks or months, thus reducing the frequency of their contacts with the illicit market, although taking on the additional risk of having 'stashed' drugs found in their possession. Regular heroin and high-dose methamphetamine users are more likely to buy in smaller quantities and generally use up their purchases almost immediately.
Illicit drugs are not equally available to all drug users. Most individuals who have reliable contacts to obtain cannabis do not know—or care to know—anyone from whom they can purchase speed or heroin. The dealers of most drugs are understandably cautious about selling to strangers and usually require that a regular customer introduce any new purchasers to them. In the case of heroin, a dealer may ask for proof that a stranger is a user of the drug before he will sell to him.47, 254 In a study of heroin users who did not become chronic users of the drug, Schasre discovered that over one-half of the ex-users stopped taking heroin as a result of losing their source of supply.231
For some drugs such as opium and cocaine, the expense of the drug and its relative scarcity in Canada militate against establishing regular consumption patterns. Except for a few wealthy dealers and 'rich hippies' who can afford these drugs and have access to a source of supply, cocaine and opium are considered to be 'treat' drugs, consumed only occasionally in Canada when they become available.104
Although many people begin the use of sedative-hypnotics, tranquilizers or oral amphetamines through doctors' prescriptions, if regular use ensues they may be forced to resort to diverted supplies of these drugs which are purchased on the illicit market. Others may first obtain pills from their friends or the illicit market and later attempt to obtain them legally by convincing doctors to prescribe them.
PSYCHOPHARMACOLOGICAL EFFECTS
One of the major reinforcing factors which encourages repeated administrations and regular use of drugs is derived from their specific physiological and psychological effects. For example, although unpleasant first reactions to heroin are common, some users of this drug claim that their first shot made them feel the way they had always wanted to fee1.145, 253 For others, a drug may simply be a pleasant experience that warrants repetition in certain social situations. Needless to say, not everyone finds each drug experience to be immediately rewarding, and negative reactions or side effects are a major factor in discouraging repeated use of most drugs.
Because of their dependence-producing effects, certain substances require daily use once a particular level of consumption has been reached. Dependence on the opiate narcotics is considered to be the 'classical' case of drug dependence, and a great deal of research has been conducted to determine the etiology or cause of this condition. (See Appendix D.2 Motivation and Other Factors Related to Opiate Narcotic Use.)
In the mid-forties, Lindesmith developed a theory of opiate dependence which he proposed would explain all cases. He concluded that opiate dependence occurs when an individual learns the meaning of withdrawal distress and consciously uses an opiate to relieve these symptoms or prevent them from occurring.15' After tolerance has developed, the organism requires the drug to function smoothly and, if it is not regularly administered, withdrawal symptoms of varying intensity are experienced. The appearance of these symptoms is crucial to Lindesmith's argument. If they are misinterpreted as some other ailment (a common occurrence when opiates have been medically administered in hospital and withdrawal discomfort is interpreted as a result of the original pathology) dependence does not occur. Similarly, persons who have been experimenting regularly with illicit heroin may interpret their first withdrawal symptoms as a common cold or the flu.145 It is only when an individual experiences the distress, realizes or learns that it is due to the absence of opiates in his body, and administers the drug to relieve his condition, that the complex of attitudes and behaviour which constitutes dependence appears. According to Lindesmith, it is at this point that an individual first comes to see himself as an opiate dependent.
Whereas drug use is generally believed to be sustained by the positive, euphoric effects of the substance, Lindesmith's work suggests that dependent drug use is also negatively reinforced by withdrawal avoidance. In other words, dependent drug use may be seen as a form of continuous self-medication or anticipatory self-medication.192 There is some difference of opinion about which drugs, at what use levels, can be said to be used this way rather than solely for their euphoric effects, but we assume that avoidance of unpleasant withdrawal symptoms is an important element of some levels of tobacco, alcohol, amphetamine, barbiturate, opiate narcotic and other drug use, especially, but not only, at daily levels-of-use.
Although the onset of physical dependence has a profound effect on use patterns and life styles of certain drug users, it is not a factor in the drug-taking behaviour of the majority of regular users of most drugs. For these, the frequency with which they indulge and the quantities of the substances involved are regulated by social interaction and normative restraints which are developed over time.
SOCIAL FACTORS
In an earlier section of this appendix we explained that initial and occasional non-medical drug use, like many other activities, is usually learned in a social context. In many instances, regular drug use patterns also become established and reinforced through social interaction. For example, an individual who is using cannabis, LSD or some other hallucinogen from time to time may acquire more friends who use these substances. This increases the likelihood that he will use more often and under more diverse circumstances. With an increasing number of opportunities to use and purchase drugs, the occasional user may be encouraged to use a drug more frequently and may eventually establish a regular use pattern by which he determines which situations are appropriate for cannabis or LSD consumption and which ones are not, as well as the amounts to use to maximize the effects desired in specific instances. He may come to believe that cannabis use increases the enjoyment of eating and make it a regular pre-dinner ritual in the same way that others will enjoy an aperitif. He may be encouraged to take LSD during an excursion to the country and decide that this experience is much more rewarding than the use of hallucinogenic drugs in the city and should therefore be restricted to rural settings. On the other hand, he may determine that his friends or acquaintances seem to use certain drugs indiscriminately or to excess, and decide to limit his use to specific recreational contexts. A similar process can be observed with persons who decide, through interaction with friends and acquaintances, what situations are appropriate for drinking alcohol, inhaling solvents or taking a number of other substances.
The influences stemming from the drug taker's social milieu which will eventually help to determine his pattern of regular drug use can be summarized briefly as follows:
1. Information. Friends and relatives may offer information on situations in which certain substances may be used for specific purposes. For example, it may be suggested that cannabis or LSD would increase the enjoyment of certain movies or concerts or that an over-the-counter or prescription drug can be used to self-medicate adverse drug effects or potentiate the effects of other drugs.
2. Example. The occasional user may learn by watching the behaviour of his peers what sorts of situations are appropriate for certain kinds of drug use, and what levels of use can be deemed excessive. Others may show by their example that no observable harm or disruption is likely to result from certain levels-of-use.
3. Ideology. Participation in drug-using groups provides supporting ideologies which neutralize some of the negative opinions and attitudes surrounding illicit drug use and provide positive reinforcement and justifications for drug-taking behaviour. For example, cannabis users commonly rationalize their behaviour through the belief that legal substances such as alcohol and tobacco are much more harmful and that smoking cannabis is a minor vice in comparison.13
4. Opportunity. The more people in the environment who use drugs on a regular basis, the more likely it is that opportunities to use will arise at times when the individual may not otherwise have thought of consuming a drug, and that he will discover more sources of supply of illicit drugs.
PSYCHOLOGICAL FACTORS
Although levels-of-use are often largely determined by interaction with friends and relatives, certain people evidently establish regular use levels at variance with those of their peers or seek out peer groups which have quite different patterns of non-medical drug use. The personality variables which may affect these decisions are discussed elsewhere in this report (see Appendix D Motivation and Other Factors Related to Non-Medical Use). It is sufficient to mention in this context that there are numerous personality factors and events in the personal life histories of some non-medical drug users which help to explain their regular use patterns as well as the inclusion of certain drugs in their pharmacological repertoire.
PATTERNS OF REGULAR DRUG USE
Patterns of non-medical drug use are numerous and varied, depending on the substances involved, their legal status and availability, their psychopharmacological effects, and a number of other factors. In addition, most substances are used in various ways by different people or by the same individuals over time. In the following pages we delineate three major types of regular non-medical drug use: functional, recreational, and dependent. Although each of these categories will be described separately, they are not to be understood as discrete types. Some drugs, alcohol for example, may be used in all three ways. Some people may use a specific drug in one or more of these ways at the same time or gradually shift from one pattern to another over a period of time. This typology does not necessarily constitute every possible drug use pattern, past and present, but is designed as a framework within which the major patterns of non-medical drug use may be described.
Functional drug use involves the consumption of a substance with the specific intention of utilizing one or more of its physical or psychological effects for reasons other than the pleasure or euphoria which the drug may provide. Some drug use may be considered functional in that it facilitates social interaction. However, for our purposes, instrumental or functional drug-taking behaviour will refer to those patterns of use in which the primary intention is to increase task-oriented efficiency or to relieve unpleasant mental or physical conditions. Functional drug use, then, is individual rather than social and specific goal oriented rather than recreational. Recreational drug use, on the other hand, encompasses those non-medical drug-taking activities which are primarly oriented to the pleasurable psychological effects of the substance and are usually restricted to social activities and leisure hours. Dependent drug use usually involves a degree of loss of control over use levels and a strong compulsion to use a drug; thus use may occur in any setting, regardless of the social situation or the immediate mental and physical state of the user.
FUNCTIONAL DRUG USE
Task performance. Drugs of the stimulant category are commonly used with the intention of increasing alertness in task performance. The most common of these are caffeine (which is consumed in coffee, tea, cola beverages and over-the-counter `wake-up' preparations) and the nicotine in tobacco products. Although coffee and tea are also used in a recreational context, their effects are employed for stimulation, both consciously and unconsciously, by most users.33 The well-established institution of the 'coffee break' is usually a social occurrence, but the substance consumed also performs secondary energizing functions.
Stimulants are sometimes used by members of certain occupational groups whose jobs require intense physical activity, alertness or endurance. Amphetamines and amphetamine-like substances are most commonly taken for this purpose by waiters and waitresses,104 taxi drivers and long distance truck drivers,83 104 and professional athletes.". 00. 91, 92 Students are also known to take them in order to stay awake and `cram' for final exams.21, 89, 249, 270 Certain medical practitioners have been accused of complicity in the development of this type of non-medical drug use. For example, cases have been reported of doctors who administer `vitamin shots', virtually on demand, to their patients. These injections not only contain a number of vitamin supplements, but also quantities of amphetamines.209, 210, 280
It appears that any form of mood-modifier, whether a stimulant or a depressant, can be perceived by some users to be a means of increasing task-oriented efficiency or performance. Although such use is not well documented it can be assumed that in some cases tranquilizers, barbiturates and low doses of alcohol may be used in this way. Doctors and other medical professionals who become dependent on opiate narcotics often assert that they began use in order to counteract fatigue caused by overwork."6. 277
Self-medication. Self-medication is a form of non-medical or quasi-medical drug use which involves the use of psychotropic substances to ameliorate certain mental conditions or psychological discomfort, or to treat physiological problems. Usually there is little or no medical supervision involved. Alcohol is commonly used for self-medication—a drink before dinner for its tranquilizing effects after a busy day, for example. Cannabis is sometimes smoked to relieve the secondary symptoms of a cold or the flu (see Cannabis Report). A number of over-the-counter preparations, such as codeine pills or cough syrups, antihistamines and other substances are used not only for their stated purposes but also for reduction of nervous tension or to induce sleep.
This type of drug use may originate from medical supervision; a physician may prescribe a preparation for the treatment of an allergy and the patient may use it, either consciously or unconsciously, for tension management or sedation. People who initially obtain `diet pills' to lose weight may take them to combat depression. Similarly, sedatives and tranquilizers are sometimes used for purposes not intended by the prescribing physician. It is often difficult to distinguish between medical use and this quasi-medical type of self-medicating drug use, but it is nonetheless clearly distinct from social or recreational drug use.
One of the more common forms of self-medication involves the treatment of drug effects or after-effects with the use of another drug. This type of cyclical multiple drug use is discussed in a later section of this appendix. It constitutes an important type of functional drug use as well as a major pattern of multiple drug use.
RECREATIONAL USE
Recreational drug use involves the consumption of a substance, usually in a controlled or non-compulsive manner, during leisure hours. The drug is taken for the purposes of attaining a measure of euphoria, increasing the enjoyment of other leisure pastimes or as an aid to social interaction. Although some recreational non-medical drug use is solitary, in most cases it takes place in the company of family or friends.
Social recreational drug use usually takes place among people who share ideas, attitudes and friendship in addition to their preferences in pharmacological substances. Drug use of this type usually begins in a pre-existing peer group, and regular use levels are often maintained in this same context. Some drug users (heroin dependents and high-dose intravenous methamphetamine users, for example) are likely to move into new drug-using circles when regular use becomes established, but most recreational drug use takes place in groups of like-minded people who would have been associated even if they did not use drugs regularly.
Barbiturates and other sedative-hypnotics are sometimes taken by multiple drug users in social settings, for euphoria or to potentiate the effects of other drugs. Low doses of methamphetamine or 'diet pills' may be used to stimulate or prolong social interaction. Regular use of these drugs, however, is not usually confined to recreational settings.
Sniffing glue and other volatile solvents appears to be primarily a recreational form of drug use. There is little data available on the solitary solvent sniffer and, although this pattern of use is known to exist, most of the literature describes the social use of these substances by adolescents or children within a peer group context.12, 37
Heroin is usually initially used as a social and recreational drug, but this pattern of use is likely to disappear as daily use begins. Nonetheless, not all heroin users become daily users, and some establish regular non-
dependent levels of recreational use.7, 57, 182, 179, 231, 232
In the majority of cases, regular, non-compulsive alcohol and cannabis use takes place in a social or recreational setting. These substances are usually perceived by those who use them to be aids to relaxation or communication or as a pleasant means to alter their mental atmosphere or attain a measure of euphoria. They may be used to relieve boredom or simply as a pleasant adjunct to other activities and appear to be a routine and normal part of the regular user's enjoyment of his leisure time.
Particularly in the early days of illicit LSD use, when the avowed sacramental and self-discovery qualities of the psychedelic experience were being publicized, consumption of this drug and similar hallucinogens was seen as a special event—not only for recreation but also for self-improvement and enlightenment. * However, as hallucinogen use has become more widespread, LSD, MDA and similar drugs are more often taken in recreational settings in a more casual manner, to enhance other social activities rather than as the raison d'etre of the gathering.
The use of alcohol as a 'social lubricant' is generally recognized and it is assumed by most people that the beverage is used, not solely for itself, but to stimulate social interaction and facilitate relaxation in a social context. Some groups of alcohol users, especially adolescents who are learning to use the substance, get together for the specific purpose of becoming intoxicated. However, as normative restraints develop and the consequences of excessive drinking are learned, there will be a higher likelihood that drinking will become secondary in the social context. Similarly, the 'pot party' where individuals gather specifically to become intoxicated may apply to some groups of new users, but as cannabis use becomes integrated into the life style of the user, it will usually become an adjunct to the ongoing social activity in the same way as recreational alcohol use is generally conceived to be.187 In any case, most non-medical drug use has its genesis in social groups, and continues to be a social and recreational phenomenon.
DEPENDENT DRUG USE
Once dependence on a drug is established, a pattern of daily—or more frequent—use, regardless of the social situation or the mental or physical condition of the user, will usually begin. Most people who use dependence-producing drugs know that others have lost control of their level of consumption, but few believe at the outset that it will happen to them. Becoming dependent on a drug is usually a gradual process throughout which an individual believes that he has control over his level-of-use while, in fact, the intervals between administrations of the drug become increasingly shorter. During the early stages of dependence, most users would claim that they could 'stop anytime'.
Tobacco dependence is probably the least traumatic as well as the most common form of drug dependence in Canada. Smoking is widely practised and tolerated and readily becomes associated with many events in the user's daily routine: with coffee, after dinner, in various social settings. Many tobacco smokers, in fact, may smoke on a daily basis for a protracted period of time without realizing that if use were discontinued withdrawal effects and craving would be experienced.33
Dependence on alcohol is usually slow to develop, and during the beginning stages of use the pre-alcoholic's drinking behaviour may be indistinguishable from that of his peers. However, Jellinek suggests that the pre-alcoholic may find the beverage to be more rewarding for tension release than do other drinkers.125 A typical pattern of becoming an alcoholic involves daily use at increasing dosages and perhaps, after a period of months or years of heavy use, the occurrence of blackouts. Sometime thereafter, morning drinking will begin, and the individual and those around him will become aware that he has lost control of his drinking behaviour. This process may take many years, although in some cases it may develop quite quickly, in response to a personal life crisis, for example.196
Although most 'problem drinkers' are involved in a daily use pattern at high-dose levels, there are several "species" or types of alcoholism.'25 One of these, which may be called "periodic alcoholism", entails occasional, but severe drinking bouts. These "habitual symptomatic excessive drinkers"163 may consume more alcohol over time than do daily drinkers, but they do not exhibit the same degree of loss of contro1.125 Such spree drinking may be just a stage in a career of alcoholism, but some individuals remain at this level and do not become daily dependent drinkers.
It seems, therefore, that not all patterns of use which involve a compulsive relationship between the user and his drug of choice require daily use over long periods of time. Patterns of daily as well as spree use of amphetamines have also been observed. One type of intravenous methamphetamine user encountered by Commission field workers maintained a relatively constant and very high daily consumption level."3 However, the more common `speed freak' pattern consisted of a series of continual 'runs' and 'crashes'. This latter pattern involved daily use at increasing dose levels for periods of a few days to a week. When use of the drug was terminated, a withdrawal phase characterized by physical exhaustion and extreme irritability and depression ensued. The most popular and common remedy for the unpleasant symptoms of this 'crash' was a new injection of amphetamine, and the 'run' would begin again.
Dependence on the opiate narcotics, particularly in their more potent forms, usually develops much more rapidly than dependence on alcohol. For those who eventually do become dependent, the period between first use and daily use of heroin usually varies from a few months to about a year.i17. 212 Dependent use is most often preceded by a period of social and recreational use. At some point, use becomes more frequent, both socially and in private, perhaps, in the latter case, to cope with stress or tension.204 Almost invariably, the user first becomes aware of his dependence when he experiences withdrawal symptoms and learns that they can be immediately relieved by the administration of an opiate.117, 151, 223
Sedative-hypnotic dependence usually results from medical prescriptions of these drugs. A general practitioner who does not fully appreciate the potential dangers of these drugs may provide his patient with a refillable prescription or the patient may go from doctor to doctor, complaining of the inability to sleep and, thereby, obtaining multiple prescriptions. Some alcoholics have been known to become dependent on sedatives. Barbiturates, purchased on the illicit market, are sometimes used by heroin dependents, and in later years, when their ability to support a heroin habit declines, some of these persons become dependent on these less expensive pharmaceutical substitutes.", 109 Although youthful multiple drug users are known to occasionally take sedative-hypnotics (particularly barbiturates and methaqualoncontaining substances), few cases of dependence in this population have come to the attention of the Commission. Should the use of these substances continue to diffuse, however, a pattern of youthful dependence on sedatives may emerge in the future.
PATTERNS OF MULTIPLE DRUG USE
In recent years there has been a growing social awareness of and concern about 'multiple drug use' or 'poly-drug use'. Although this pattern of drug use is sometimes seen as new and, perhaps, exotic, the consumption of a number of psychoactive substances is not a recent development or one confined to a specific segment of contemporary society. Broadly conceived, multiple drug users are those who ingest a number of psychoactive substances, either simultaneously or at different times. Accordingly, a person who uses alcohol, tobacco and caffeine is a multiple drug user, as are those who consume a variety of illicit substances apart from or in addition to these. Certain patterns of multiple drug use, however, are seen as more dangerous or more cause for concern than others, depending on the drugs involved, the levels and frequencies of use or their relative potential for harm.
In the literature of multiple drug use, the concept is often reserved for only those who use more than one illicit drug in a non-medical context. This can lead to certain conceptual ambiguities—where under-aged high school students use alcohol and tobacco, for example—in addition to imposing limitations on interpretations of the data and the cogency of the research results. A meaningful operational definition of multiple drug use should specify what drugs are under consideration as well as the context of use. For our purposes, we are interested in patterns of multiple use of any substances used in a non-medical context.
A second dimension which must be considered in arriving at a workable definition of multiple drug use is the frequency with which psychoactive substances are used and the dosages employed. Most multiple drug use studies employ a minimal definition: the multiple drug user is one who has 'ever used' more than one substance. Such a definition appears to be quite uninformative and unsatisfactory since individuals who have had little experience beyond the experimental stages of use are included with chronic, high-dose users (see Annex 1). Definitions of multiple drug use, therefore, should specify at what levels of regularity and frequency the substances in question are employed and, if possible, supply relevant dosage information.
Multiple drug use may be examined from two perspectives: as either concurrent or sequential patterns of use. In the former case, the emphasis is on the organization, patterning and interrelationships of the various substances in the life of the user at a particular time. The second perspective, that of sequential multiple drug use, involves the study of the temporal order in which each drug comes to be used or added to the pharmacological repertoire of the user. The concept of 'progression' is often subsumed under the general rubric of multiple drug use. However, sequential drug use may be distinguished from 'progression' insofar as the latter concept assumes that there is a hierarchy of drugs ranging from 'soft' to 'hard', weak to potent or less harmful to more dangerous, and that there is a tendency for drug users to move up this hierarchy to 'stronger' drugs. The emphasis of the term `sequential' is on the movement from one drug to another without necessarily implying increasing danger or movement to more potent substances, both of which are connoted by the word 'progression'.
CONCURRENT MULTIPLE DRUG USE
Patterns of concurrent multiple drug use may be distinguished as intermittent, simultaneous, cyclical or interchangeable.
When two or more drugs are used, but not at the same time, this pattern may be called intermittent multiple drug use. Thus, an individual may use cannabis and LSD, but not in the same situation. Intermittent multiple drug use often involves two quite different use patterns: the functional use of amphetamines, for example, may not overlap with the recreational use of other substances.
Simultaneous multiple drug use, on the other hand, may be defined as the ingestion of two or more psychoactive substances in such close conjunction that the effects of the drugs are acting on the organism at the same time. Some simultaneous patterns involve the deliberate consumption of two or more substances to obtain a specific interaction effect. An illustration of this is the `speedball', an intravenous combination of heroin and cocaine or methamphetamine. Others, however, may simultaneously use two or more drugs without being aware of their potential interactive or additive effects. For example, a daily user of a prescribed sedative-hypnotic may also use caffeine, alcohol or other drugs without taking into account his ingestion of the former.
When one drug is used as a substitute for another with similar psychopharmacological properties, interchangeable multiple drug use may occur. Thus heroin users may purchase barbiturates or, preferably, methadone when heroin is in short supply. Although they may find alcohol distasteful while using heroin, heroin users often drink to excess when abstinent from opiates 2b3 A number of interchangeable drug use patterns are further discussed in C. 4 Patterns of Use, "Social Theories of Multiple Drug Use".
Cyclical multiple drug use is the ingestion of two or more substances consecutively such that the later ones modify or counteract the terminal effects of the earlier ones. Those who have used alcohol to excess are familiar with the 'morning after' syndrome which often follows. 'Hangovers' are commonly treated by liberal amounts of caffeine, in the form of coffee, tea, or cola beverages. Codeine pills are sometimes used to relieve the accompanying aches and pain, and in some cases `wake-up pills' or amphetamines are used to counteract post-alcohol drowsiness.
Cycles of stimulation and sedation are a common multiple drug use pattern. 'Diet pills' or other stimulants are sometimes used to banish the `morning after' effects of sleeping pills. On the other hand, sedatives or alcohol may be used to induce relaxation or sleep after the effects of amphetamine begin to fade. 'Speed freaks' occasionally use barbiturates or heroin, if they are available, to self-medicate adverse withdrawal symptoms after a 'run' of high-dose, intravenous methamphetamine use. Commission research has confirmed that this form of cyclical multiple drug use has lead some speeders to a preference for heroin because of its capacity for stabilizing and tranquilizing without the adverse physical and psychological effects of the amphetamines.'"
Some of the recent concern over concurrent patterns of multiple drug use has been given impetus by what is called the 'garbage head syndrome'. In the spring of 1972, Commission field workers discovered that observers of the youth scene were becoming increasingly aware of this problem in cities across Canada.'" 'Garbage heads' have been described as the archtypal and extreme multiple drug users who consume a dazzling array of substances sequentially or in combination, with little regard to the consequences beyond `getting stoned'. With the recent lowering of the legal drinking age, much of this multiple drug use activity has been observed in pubs or taverns where large quantities of alcohol are used in combination with one or more other drugs. Often these young people will have little or no idea what drugs they have consumed, stating that someone offered them a pill of a certain colour and promised that it would get them 'stoned'.
Some observers believe that the 'garbage head' is likely to be a transitory or short-lived drug use pattern in most cases. When some adolescents begin to use alcohol, they go through a period of excessive use, drinking to the point of drunkenness and sickness. Eventually, most of these develop normative restraints and the ability to control their intake and their behaviour under the influence of alcohol. The 'garbage head syndrome' has been observed most frequently in provinces which have recently lowered the drinking age. It appears that whereas most high school aged drinkers and illicit drug users formerly experimented with these substances out of the public eye, they are now readily observable in drinking establishments. It seems reasonable to assume that, particularly after a number of unpleasant experiences, most `garbage heads' will exert some control over their drug intake and settle into more moderate regular or occasional patterns of consumption.
SEQUENTIAL MULTIPLE DRUG USE
Various 'progression' or 'stepping-stone' theories have been advanced to explain why individuals, having established the use of a particular drug, will experiment further with other psychotropic substances. In order to understand the genesis of these theories and how they came to have currency today, a brief historical introduction follows.
The Prohibitionists in the United States were the first to propose any kind of progression hypothesis:
The relation of tobacco, especially in the form of cigarettes, and alcohol and opiates is a very close one.... morphine is the legitimate consequence of tobacco. Cigarettes, drink and opium is the logical and regular series."'
Cannabis was not included as one of the drugs that was involved in this progression as it was not until the 1930s that consumption of marijuana became sufficiently widespread in the United States to receive public attention. The idea of the cannabis-heroin progression was first presented in 1931 by a Prohibitionist physician:
[Marijuana users easily] become engulfed in the abyss of drug addiction, and end their miserable existence either on the gallows, or in penal institutions and insane asylums. The moral and physical resistance to narcotics and alcohol is not only weakened but often destroyed in persons of stabilized personality, who are addicted, even to a moderate degree, to marijuana."
During the thirties and forties, the notion of the marijuana to heroin progression appeared in a few works on cannabis, but there was virtually no supporting evidence that such a relationship existed. Moreover, there was little consensus among these writers as to what factors 'caused' this alleged progression.158 At this time, those authorities most familiar with drug use—police officials and medical professionals—strongly denied that such an escalation existed.
After the Second World War, there appeared to be an epidemic increase in the extent of heroin use in the United States, particularly among young men of racial minority groups in large urban areas. The popular press suggested that this new heroin 'epidemic' and the 'new breed of addict' had come to opiate use through the use of marijuana. The assertions that cannabis was an extremely dangerous, addicting and crime-inducing substance were beginning to lose credibility at this time due to the findings of the La Guardia Commission and a number of psychiatric studies which appeared between 1944 and 1946.35, 55' 85, 181' 185 Some observers of the heroin scene came to the conclusion that cannabis use, per se, may not be as dangerous as they had thought originally, but that its use led to heroin and was thus responsible for the 'new breed' of user.
An examination of the social history of opiate use in North America reveals that the 'new addict' was, in fact, not a new phenomenon. The postwar users were seen to be quite different from the middle-class, middle-aged, medically dependent population of the turn of the century.256 However, the use of opiate narcotics by young delinquents was well established prior to the introduction and diffusion of cannabis. Although thousands of people who would otherwise be considered to be 'respectable' were dependent on patent medicines and home remedies containing opiates, there were also a number of 'underworld' denizens—gamblers, vagrants, and prostitutes—who were habituated to opium smoking or dependent on morphine. By the 1920s, when legal access to opiates had been restricted, a number of clinics were established in the United States to supply maintenance doses of opiates to those who were still dependent.15°, 234 One of the reasons why these clinics were eventually forced to close was the publicity given to the 'criminal element' in their patient populations.245 Apparently, dependence on opiate narcotics was quite common among the young, the socio-economically disadvantaged and the 'underworld' before the onset of widespread cannabis use.71, 136, 140, 250 There is good reason to believe that the post-war 'epidemic' was actually a reflection of a growing trend that had its roots in the changes which took place at or before the turn of the century and had only been interrupted temporarily by the war. The increase in heroin use in the late forties, according to this view, was due primarily to the re-establishment of overseas shipping and transportation routes, allowing once more for extensive illicit distribution of heroin.158
Once established in the late forties, concern about drug progression, specifically the escalation from cannabis to heroin, continued. However, with the diffusion of the use of LSD, barbiturates and amphetamines in the 1960s, the concept of 'progression' was broadened to take some of these substances into account, and thus the movement from cannabis to heroin is now often considered to be only one of a number of sequential drug use patterns.
Discussions of the relationship between cannabis use and the use of opiate narcotics may be found in Appendix A.2 Opiate Narcotics and Their Effects as well as in the Cannabis Report. In the latter document, the Commission majority acknowledge that certain individuals would engage in heavy multiple drug use whether they used cannabis or not, but asserted that,
... it is reasonable to assume that many would not engage in certain kinds of drug use if they did not use cannabis."
They concluded that, although cannabis use may play some role in influencing subsequent use of other drugs, sequential multiple drug use was too complex a process to assign a strict causal significance to one factor or one particular drug.
A number of retrospective studies of heroin users and follow-up studies of marijuana users are also discussed in the Cannabis Report and Appendix A.2 Opiate Narcotics and Their Effects of this report.9, 41, 54, 94, 199, 215
These studies have a number of methodological problems, the most important of which is their concentration on the most 'heroin-prone' populations, such that the results may not be generalized to the cannabis-using population as a whole. On this subject, Appendix A.2 concludes:
Specific pharmacological properties of marijuana (or any other drug) which might lead to a need or craving for other drugs have not been discovered. It would appear that dynamic and changing social and personal factors play the dominant role in the multi-drug-using patterns repOrted, and that the specific pharmacology of the compounds involved is secondary.
Historically, a number of varied, and often discrepant, theories have been proposed, all of which attempt to demonstrate that cannabis use is causally related to the subsequent use of other drugs. Although these explanations have differed radically in content as well as their level of sophistication, they will be presented, in the following pages, as a framework through which some understanding may be gained of the numerous mechanisms that may influence sequential drug use patterns or the movement from one drug to another.*
Psychopharmacological effects theories. The first and most classic type of explanation for the progression from marijuana to other drugs is the psychopharmacological effects model. Although these theories vary somewhat in their level of sophistication, the majority are naive and overly simplistic accounts of sequential drug use patterns. All of them single out the effects of cannabis as the determining cause of the progression.
One alleged effect of cannabis that was postulated to lead to heroin use was a loss of self-control or will power which was said to make the user more vulnerable to the use of other drugs.157 However, although a loss of self-control was alleged, no attempt was made to verify its existence.
Another explanation postulated a tolerance-disillusionment type of progression mechanism. It suggests that the initial 'kick' that marijuana users experience tends to wear off over time due to tolerance. The user then looks for a more powerful substitute. It has also been proposed that cannabis users expect ever-increasing pleasurable effects from the drug and are thus compelled to turn to stronger drugs to satisfy their "taste for drug intoxication"." This particular theory did not specify why it was only cannabis that could create a taste for intoxication rather than alcohol or other drugs used prior to cannabis. A variation of this general theme suggested that the cannabis user becomes psychologically dependent on the drug and that this paves the way for his subsequent use of heroin.'"
As we observed in the Cannabis Report, there has been no empirical verification of these theories, and no evidence that the effects of cannabis per se can be said to encourage later heroin-using behaviour.43 If the psychopharmacological effects of cannabis do in fact influence the user to turn to stronger drugs, we would expect a relatively constant rate of progression from marijuana to the use of heroin or other drugs.* However, there is no evidence to date which would suggest that all cannabis users—or even all cannabis users at a particular level-of-use—are equally likely to use other drugs in the future.29, 98,126
In addition, if one examines the processes by which people come to use heroin, it is difficult to single out cannabis use as a determining factor. There is no evidence to suggest that first use of heroin occurs when the individual has little power of resistance due to the direct effects of cannabis. Whether someone experiments with heroin or not depends on various aspects of his life style, his attitudes to the drug, as well as his past experience with heroin users. Finally, it is evident that the factors which influence first use or experimentation with heroin may be quite different from those which lead to opiate dependence (see Appendix D.2 Motivation and Other Factors Related to Opiate Narcotic Use).
Since cannabis is not a necessary precursor of heroin use (before 1965, few heroin users in Canada had taken cannabis prior to opiates),117. 194, 253 the most we may assume is that the effects of the drug could only be influential on certain cannabis-using persons, and that others find another path to heroin dependence. This type of thinking brought theorists to the point where they began to look at personality variables for the motivating forces leading people from cannabis to the use of other drugs.
Personality abnormality theories. The basic assumption of this kind of theory is that the majority of those who progress from the use of cannabis to the use of other drugs are, to varying degrees, psychologically disturbed. It is sometimes suggested that the use of cannabis is, in itself, indicative of an underlying personality problem and that those with more severe problems will not find cannabis to be a sufficient solution. They will, therefore, go on to heroin use (or the use of other drugs) in search of a more adequate problem-solving drug.
Psychological investigation of multiple drug users is usually conducted on those subjects whose patterns of drug use are assumed to be a cause for concern. Most observers, for example, would not consider daily use of alcohol, caffeine and tobacco to be indicative of an underlying personality disorder because of the legal status and general social acceptability of these drugs. Attention, therefore, has largely been focussed on chronic or high-dose drug users and those whose multiple drug use patterns include the use of
illegal substances.64, 113, 141, 168, 284
Although continuing to yield interesting data, psychological studies of multiple drug users do not provide us with precise information regarding the role of psychological variables in the choice of drugs in a drug-using career. Most of them are characterized by the same methodological problems as those studiec which have attempted to discover the psychological dynamics of heroin lependence, the 'addict personality', or the 'alcoholic personality'.38, 87 While some types of heavy multiple drug use would seem to indicate personality problems, many multiple drug users would clearly be diagnosed as psychologically normal. The relationships between psychological variables and the use of opiate narcotics, amphetamines and hallucinogens is further reviewed in Appendix D Motivation and Other Factors Related to Non-Medical Drug Use.
Social theories of multiple drug use. Although it is reasonable to hypothesize that increasing use of stronger drugs reflects the existence of severe personality disorders in some cases, other evidence suggests that factors in the social background and environment of the drug user may influence his particular sequential drug use pattern. Patterns of drug use reflect different meanings attached to drugs by different groups of individuals, and drug-taking behaviour is interwoven with other activities of group life.3 Orientation to and eventual selection of drugs, as seen from a sociological perspective, reflects a number of factors such as availability, information, and other influences in the immediate social environment.
With the use of one drug comes an increased likelihood of meeting others who use that drug and, perhaps, use other drugs, as well. That cannabis users are more likely than non-users to have drunk alcohol suggests that alcohol users have a greater chance of having friends who would be willing to offer cannabis to them. Similarly, the use of cannabis may introduce an individual to a wider range of persons who use a variety of legal and illegal drugs, and it has been hypothesized that this 'drug subculture' is a significant determinant of further drug use. However, the illicit 'drug subculture' is by no means a homogeneous entity and is better characterized as a mosaic of small `drug subcultures'. Multiple drug users may have in common the use of one or more illicit substances, but they differ in terms of patterns of multiple drug use and in their orientation and attitudes to specific kinds of drug use. A number of studies have confirmed that the choice of drugs which are to be included in the pharmacological repertoire of the drug user appears to be mediated by the immediate social and cultural environment.3, 29, 56, 126, 141, 195
Many of the same factors which help to determine regular drug use patterns also influence the numbers and kinds of drugs included in any variety of multiple drug use. As we have seen, availability of illicit substances plays an important role. Some degree of interchangeable multiple drug use is alleged to occur when an individual's current or favourite drug becomes unavailable or prohibitively expensive. The importance of this factor was emphasized by the R.C.M. Police in a brief submitted to the Commission:
... the scarcity of marihuana would act as a catalyst in introducing the drug user to stronger drugs which may be available, such as L.S.D., amphetamines, barbiturates and heroin....'
During the summer of 1969, a marijuana shortage was reported in the United States, and a study was undertaken to investigate its effects.'" Interchangeable multiple drug use patterns were reported by over three-quarters of one sample and by 84 per cent of another sample. The most common substitutes were alcohol and hallucinogenic drugs.
Some juveniles may use cannabis as a substitute for alcohol when it is more readily available to them in their immediate environment.3 It has also been suggested that volatile solvent users actually prefer alcohol as an intoxicant, but use solvents because they are too young to have ready access to alcoholic beverages.* It is evident, therefore, that sequential multiple drug use is sometimes encouraged by scarcity of the drug of choice and the substitution of a different intoxicant.
In our earlier discussion of the process of becoming a regular drug user, access to the illicit marketplace was emphasized as an important factor. Such access may also play a role in introducing an individual to new drugs which he might not have previously used. Some observers feel that the illegal status of cannabis and the consequent fact that one must resort to the illicit market to purchase supplies may introduce cannabis users to a wider variety of illicit substances:
By transacting with, and making friends with, the marihuana "dealer" ... one's values and attitudes toward drugs and drug-taking, will be influenced in the direction of an increased willingness to try and use a wide range of drugs. Moreover, one's dealer, offering as he does a pharmacological feast, provides opportunities to use other drugs.'
Heavy use of cannabis has been proposed as one condition that will lead to the non-medical use of other drugs. However, there are a number of intervening variables which come between heavy cannabis use and subsequent multiple drug use. The more cannabis used by an individual, the more likely it will be that he becomes involved in both buying and selling marijuana or hashish. Furthermore,
Buying and selling push the individual into social relations that alter his conception of himself regarding drug use and provide opportunities for involvement with other kinds of drugs. The fact that the individual has bought and sold marijuana means that he has had contact with other individuals who are likely to be heavily involved in drug use and who define drug use in favorable terms.'
Thus, closely related to the buying and selling of cannabis is the contact with new acquaintances and friends who use other drugs and define such use positively.25, 126
The original correlation between frequency of use [of marijuana] and the use of dangerous drugs is largely due to involvement in selling drugs, not use itself .... Thus the causal link between marijuana use and the use of dangerous drugs does not appear to be the use of marijuana at all. Use of marijuana is merely an external manifestation of something that underlies it—namely, involvement with and in a drug-using subculture, especially in the form of buying and selling illegal drugs, and having friends who use other dangerous drugs."
We come, therefore, once more to the importance of the drug use patterns of one's peers in introducing an individual to any kind of drug use.
Johnson concluded that the less socially accepted a drug is in the immediate social environment, the more likely it will be that an individual will need to acquire intimate friends who use it before he himself will experiment with the drug.126 The cannabis users in his sample used the `harder' drugs of which their subculture or circle of friends approved. Without the acceptance of friends, the chances of cannabis users moving to other drugs was considerably decreased.
The influence of set and setting on multiple drug use. Some recent theories of sequential drug use have combined both psychological and sociological orientations. The 'set and setting' theory emphasizes individual circumstances, suggesting that it is an individual's psychological 'set', or complex of attitudes towards drugs, in combination with his particular environment, or `setting', which determines subsequent drug use. This argument has been extended to suggest that some drugs may be no more than placebos, or that the psychopharmacological action of the substance is unimportant in comparison to the influence of set and setting.271
One study of juvenile multiple drug users discovered that within a single lower-class neighbourhood there co-existed a variety of adolescent drug-using patterns.29 These patterns differed markedly from one another in terms of the types of drugs used, the degree of involvement in drug use, and in the attitudes and orientations of the users prior to and after first experimentation. The study concluded that there were different life orientations and both drug and non-drug career lines along which adolescent users could pass, and that these would largely determine subsequent adult drug use behaviour as well as adult social adjustment.
The 'set and setting' approach to understanding multiple drug use patterns appears to be a most fruitful one. It is evident that there are strong relationships between the use of all drugs; that is, the individual who has used any one drug (including alcohol, tobacco and caffeine, as well as more exotic substances) has a higher likelihood of having used other substances and is also more likely to be favourably predisposed to experiment with other drugs in the future. Any non-medical drug use may contribute to or enhance a drug-taking set and may also introduce the user to a wider setting in which further drug use is accepted or positively encouraged. There are a variety of factors which contribute to a positive set towards drug use, but which are insufficient predictors of subsequent multiple drug use patterns unless a suitable setting, with drug availability and reinforcement from others, coincides with it.
For further information about the relationships between different kinds of drug use, the reader is referred to Annex 1 Extent of Multiple Drug Use of this appendix, and Appendix A The Drugs and Their Effects.
LIFE STYLES OF REGULAR DRUG USERS
Some levels of regular drug use have profound effects upon the social and economic relationships of users. Others, such as the use of coffee, tobacco and certain over-the-counter preparations, have little or no immediate influence, although long-term medical complications may occur. Daily use of sedatives, oral amphetamines and tranquilizers at moderate dosages may eventually interfere with day-to-day functioning, but high-dose use is generally responsible for most serious difficulties.
At light to moderate dose levels, regular alcohol use is both socially acceptable and unlikely to present problems for the user. In fact, in some social and economic positions, it may be more difficult to be an abstainer than a drinker. Moderate use may cause some degree of economic inefficiency due to hangovers or other potential medical problems, but is unlikely to disrupt social and familial relations as long as the user's behaviour under the influence of alcohol and his particular level-of-use are acceptable in his social milieu At dependent or high dose recurrent use levels, alcohol usually produces extreme social, economic and family disorganization, probably more so than any other kind of drug dependence. Since alcoholism usually develops in middle age, it is likely that the alcoholic will have a career and family which will suffer as a result of his drinking habits, whereas heroin and high-dose methamphetamine dependence tend to occur among younger, unattached people. The consequences of the onset of dependence in the latter cases tend, therefore, to have less far-reaching disruptive effects.
The use of cannabis at social or recreational levels need not have any more effect on the life style of the user than similar use of alcohol, as long as use remains undetected by law enforcement officials. When cannabis first became popular among certain youthful North American populations, its use appeared to reflect a distinct kind of life style, most commonly termed 'hippie'. However, as the use of cannabis has diffused, it has become evident that quite ordinary, traditionally employed persons consume it in recreational settings on a regular basis, and that cannabis use, although a concomitant of the 'hippie ethos', does not necessarily imply attitudinal or behavioural changes.
The case of LSD, mescaline and other psychedelic drugs is somewhat similar. When LSD was first gaining in popularity, both observers and users themselves claimed that taking these substances would change an individual's attitudes, outlook and style of life. The vanguard of the psychedelic movement found LSD use to be profoundly enlightening and the revelations experienced under the influence of the drug were believed to have lead to a reevaluation of their lives and the adoption of new behaviour patterns and levels of social interaction. However, when use spread to younger or less philosophically-oriented populations, it soon became evident that this process was not inevitable. Less introspective or more hedonistic users were consuming these drugs for their euphoric effects rather than for personal, philosophical or religious purposes. Many of those who had sought personal change through these drugs were disappointed and stopped using them or began to use them more casually. For most, LSD became just another 'stone',
In the early stages of use, both heroin and speed users usually have one source of supply of the drug, through the friends who introduced them to it. Those who continue to use these drugs discover that, due to the vagaries of the market, new contacts must be made.268 Although some social relationships with non-using friends will be maintained,177 it is likely that a gradual separation will be made from some of these as heroin or speed use becomes more regular, and new friendships will develop through the illicit market (see Appendix D Motivation and Other Factors Related to Non-Medical Drug Use). When heroin or speed use becomes a daily affair, the ritual of the `fix' (administering the drug) becomes the central feature of the activity of everyday life, and many heroin dependents and compulsive speed users spend the majority of their waking hours searching for drugs or the money to purchase them.20, 103, 162, 247, 268
Much of the isolation of the speed user from conventional and non-speed society is due to the constant chatter, or 'rapping' of the speeder, his hyperactivity and paranoia. The pharmacological effects of the opiate narcotics, on the other hand, do not have such adverse influences on social relationships with non-users; however, the necessity of obtaining money to buy daily supplies of illicit heroin at inflated prices forces the user to become primarily involved in heroin-related activities and to lose contact with many aspects of his pre-heroin life. This situation does not apply to those who become dependent on opiate narcotics through access to medical supplies. A doctor or nurse who has become dependent will usually continue to function adequately in both professional and social roles, In one sample of dependent doctors, 25 per cent of the wives did not know that their husbands were dependent,277 and friends and colleagues usually do not suspect that a medical professional is using opiates until he comes under scrutiny by narcotics investigators because of his prescribing practices or because his habit begins to exceed the amount of the drug that can be obtained by quasi-legal means without detection.
Some types of regular drug use—particularly alcohol, heroin and methamphetamine dependence—often generate a host of acute and chronic medical complications. Many of these are considered in a separate appendix (see Appendix A The Drugs and Their Effects), but it is worth repeating that the use of unsterile needles is particularly likely to result in physical problems. The personal risks involved in the utilization of 'dirty points' (unsterile, barbed, or often-used needles) are well recognized by most heroin and speed users, yet it is not uncommon to observe such persons borrowing someone else's 'set of works' (syringe and needle) despite the foreknowledge that the lender may have hepatitis or venereal disease. Howard and Borges after interviewing 50 parenteral drug users in San Francisco in 1968, suggested that needle-sharing served several social and psychological functions for the participants.118 Among those functions delineated by their subjects were certain "pragmatic considerations" such as economical expedience, "sharing for the sake of sharing" (which is almost a normative imperative within some communities of intravenous drug users), providing "a sense of fraternity", as a "means of socialization" to the needle culture (novice users, particularly, are unlikely to possess their own equipment), as a "substitute for sex" (since the sexual connotations of injection are accentuated), and "gratification in self-destruction" either purposefully (masochism) or unconsciously. It should be additionally noted that, in the case of speeders, injection almost always occurs in a group setting such that one 'set of works' will be passed from user to user (much like a marijuana cigarette in a cannabis-smoking situation) and that speed dealers' rooms are ordinarily furnished with a communal needle and syringe so that clients may immediately inject upon completion of their purchase. Finally, the actual injection process itself, among experienced speeders, is highly ritualized to the point that parenteral proficiency and the ability to perform 'trick shots' has become a source of some status within this subculture.
TERMINATION OF USE
Once a particular level-of-use has been established, an individual will not necessarily stay with it indefinitely. Drug use, like other forms of social behaviour, is a dynamic process during which levels-of-use increase, decrease and, in some cases, cease altogether. In the following pages, we will present some of the factors which influence decreased use or termination of use.
Some social and recreational drug use is only experimental or occasional and never becomes established as a regular part of the individual's life style. Cannabis, LSD, speed, heroin and other drugs may be used a few times to explore their effects or because of certain social pressures, but with no commitment made to their continued use. In addition, some levels of regular or occasional use may be a part of a given social context and will cease when the social situation changes. Termination or reduction of drug use may thus occur with graduation from school, change of residence or neighbourhood, a new job, marriage, parenthood or a number of events in the life of an individual. These events may influence drug-using behaviour in several ways: by removing a person from his source of supply of illicit drugs, by replacing an interpersonal environment in which there are social pressures to use with one where use is discouraged, or simply by offering a number of substitute activities. These conditions of termination are reversible, however, and if new drug-using friends or acquaintances are discovered, or the social situation changes again, drug use may resume or increase.
Reduction or termination of use may take place as part of a general reevaluation of an individual's personality and role in society or as a commitment to other endeavours or enterprises. Some drug users become involved with political movements that do not approve of drug use. Others may stop using because of involvement with religious groups, the 'Jesus Freaks" or `Hare Krishna' movement, for example. In addition, drug use may be temporarily or permanently terminated because of a personal identity crisis which leads an individual to question his values and behaviour in general. Some users may temporarily refuse to use cannabis or LSD, for example, because they feel they 'are not together enough to handle it' for the time being.
In an earlier part of this appendix, we suggested that most use of LSD and similar hallucinogens is usually self-limiting and transitory. Ex-users often cite 'bad trips' or uncomfortable experiences as their reason for stopping. This rationale is sometimes offered by ex-cannabis users as well. Others claim that they are no longer learning anything from LSD or that it is no longer possible to obtain unadulterated or 'pure acid'. The growing sensitivity of some illicit drug users to the dangers of pollution, chemical fertilizers and food additives is sometimes generalized to the drugs they consume, although this usually results in a move away from 'chemicals' to what are alleged to be more 'organic' drugs, such as psilocybin, mescaline or peyote, rather than to complete termination of drug use. The publicity given to the possibility of chromosome damage may have convinced some people to stop using LSD; however, it appears that users and potential users did not regard this to be a real danger, or, if they did so, it was only for a short period of time.*33
In most cases, solvent use is also a transitory drug use pattern. Children and adolescents may use these substances, sometimes quite heavily, for a period of time, but it is apparent that this use is usually abandoned when they become old enough to obtain alcohol, cannabis or other more socially approved drugs with fewer unpleasant side effects.29 Ex-users usually report that they simply lost interest in these substances or became worried about their harmful effects.241 There are certain rare cases of people who continue to sniff solvents long after their friends have stopped using. This chronic pattern of use is usually solitary and compulsive.
Because task-performance functional drug use is specifically related to certain role-oriented situations, it is to be expected that it will continue on some level until the user is no longer participating in the activity. Those who are not familiar with the recreational possibilities of prescription drugs will be likely to use them only in those situations in which they feel it helps them function, but not at other times. Although students may use stimulants at exam time to keep them awake while studying, they are less likely to take them at other times or in other social settings. Similarly, members of occupational groups who utilize psychotropic substances are unlikely to use them outside of their hours of work unless they are familiar with the recreational use of these drugs or, in rare cases, have become dependent on them. For example, waitresses on the fringes of the entertainment world may well continue in their use of amphetamines or amphetamine-like drugs during nonworking hours. However, truck drivers or taxi drivers who are only familiar with their use in a functional context are unlikely to use amphetamines during their leisure hours or after changing to another occupation. Self-medicating functional drug use is bound to specific psychological and physiological conditions and is not likely to continue after the condition is ameliorated unless the user becomes dependent or learns that the drug can also be used recreationally. Finally, it should be noted that the loss of a regular source of supply may force a cessation of functional drug use. For example, the recent federal restrictions on the prescribing of amphetamines and some amphetamine-like drugs (see Appendix B.3 Sources and Distribution of Amphetamines and Amphetamine-Like Drugs) has likely reduced the availability of pharmaceutical forms of these substances and, consequently, may have reduced the prevalence of this type of use. We are not able to say at this time how these restrictions have changed patterns of stimulant use or whether users are turning increasingly to illicit supplies of these drugs.
The following discussion will review the special problems posed by termination of dependent drug use. Accumulating evidence suggests that drug dependence does not necessarily imply continuous, daily consumption of a substance throughout the lifetime of the user. Indeed, for most so-called addicts, periods of active dependence represent only a fraction of their life-cycle. Although there is a high probability of relapse, heroin dependents usually experience intermittent periods of voluntary and involuntary abstinence.117, 185, 269 Alcoholics periodically 'go on the wagon', and many tobacco smokers make repeated attempts to rid themselves of their dependence on nicotine. In the following pages we discuss the factors which affect these cycles of abstinence and relapse.
There is little published data on the abstinence and relapse patterns of those who become dependent on oral amphetamines, barbiturates, tranquilizers or other sedative-hypnotics, and thus lengthy discussion of factors affecting termination of use is impossible. Nonetheless, there are a number of aspects of prescription drug dependence which would appear to encourage rapid cessation and discourage relapse. Most of these cases originate from legitimate medical practice, and it is reasonable to assume that medical intervention may occur at an early stage. Unlike reformed alcoholics or tobacco smokers, former users of barbiturates or `diet pills' are unlikely to be in continual interaction with current users and thus will have fewer temptations to relapse. Barbiturate dependence is often associated with heavy alcohol use, and although this complicates treatment of the condition, the pharmacological similarities of these drugs allow for a transfer of dependence. Unlike heroin or methamphetamine dependents whose lives have been dominated by drug-related activities, those dependent on prescription drugs, like the medical professional dependent on opiate narcotics, may have families or careers to turn to and need not radically change their life style to maintain abstinence. These conditions suggest that dependence on prescription substances may be less unremitting than other dependencies, although there are no available studies which test this hypothesis. Indeed, there is very little published data on termination of prescription drug dependence.
The life style of the 'speed freak' is so physically and psychologically demanding that few remain in the speed community for more than a couple of years. A few speeders learn to 'maintain', continuing to use at levels that do not interfere radically with their day-to-day activities, while getting enough sleep and nutrition to prevent profound physical deterioration, but this career pattern is rare. Other speeders may voluntarily withdraw from the life of intravenous amphetamine use, and a few are rescued by friends or relatives. For most, however, there is no place to withdraw to, and their eventual termination of speed use is dependent on their arrest or hospitalization (for a variety of ailments including malnutrition, psychosis, and hepatitis), or a change to the intravenous use of opiate narcotics or barbiturates as a drug of choice. The use of these depressants usually begins as a form of self-medication to counteract the depression and anxiety of the 'crash' at the conclusion of a prolonged speed 'run'. Some users alternate between stimulants and depressants for extended periods of time, and some of these eventually become dependent on heroin or methadone, or, in rare cases, barbiturates.
Most research on termination of drug dependence has concentrated on alcohol and opiate narcotics. We will therefore base the discussion which follows on the data drawn from these studies and insert comments on other dependence-producing drugs only where reliable information is available.
It is generally believed that it takes 10 to 20 years of drinking to become an alcoholic.125 By the time an individual recognizes that he must change this pattern or suffer progressive disorganization and debilitation, morning drinking has usually begun. Upon arising, the alcoholic drinks to relieve his hangover, continues to drink during the day to ward off shaking hands and other withdrawal symptoms and lives in fear of being unable to maintain a readily available supply of the drug.'" A major portion of the alcoholic's life is divided between the consumption of alcohol and periods of sobriety which terminate in yet another binge of drinking. Almost all conditions and activities of daily life have been associated with drinking and it is thus very difficult to maintain stable abstinence in the face of numerous drinking-associated everyday events and activities.6°, 61 This 'habit' component of alcoholism, which is independent of the specific psychological or physical effects of the drug, is present in all forms of drug dependence.
Tobacco smoking is also integrally bound to most daily activities. Abstinent smokers often discover that they are tempted to take up the drug again at social gatherings, at times of stress, after a meal or on other occasions when a certain activity elicits the memory of and desire to smoke. Some ex-smokers claim to be particularly susceptible to relapse when they drink alcohol.
The 'habit' component of heroin dependence is particularly strong. Even after long periods of abstinence, actual physiological craving may reappear.255 The smell of a burning match, which is associated with 'cooking up' an injection, or simply talking about drugs may elicit craving and even physiological withdrawal symptoms.155, 2" Stevenson and his associates discovered that for some British Columbia ex-users, a return to Vancouver or a familiar neighbourhood where heroin is sold can spontaneously produce these symptoms.253
For the 'hard core' heroin or chronic speed user, drug-taking is not only associated with a variety of states of mind, people, places and sensations as it is with alcohol and tobacco dependents, but it is also an important motivating force in the majority of his daily activities. When abstinent, he no longer must 'hustle' for money to buy drugs and many of his normal day-to-day activities are no longer necessary. Thus simply finding meaningful activities to fill up the day becomes an important aspect of sustained or successful abstinence. Although all persons who have withdrawn from a drug on which they were dependent must build up a 'tolerance for abstinence' just as they built up a tolerance to the drug and the concomitant life of dependence,4, 208 for heroin and speed users, especially, abstinence demands that a multitude of habits other than drug-taking must be broken.
It has been suggested that under some conditions it may be less difficult for the heroin dependent to discontinue the use of opiate narcotics than for the alcoholic to stop drinking.253 Alcohol is legally available and used freely in most social environments and the ex-alcoholic will be exposed to drinkers or drinking situations wherever he goes. The opiate narcotic or methamphetamine dependent, on the other hand, has the possibility of taking a 'geographical cure', by relocating to an area where these drugs are not available or where he has no connections to purchase them. In British Columbia, for example, many heroin users have sought jobs in logging, mining or other occupations in remote areas."7 This alternative may have become less possible as the availability of heroin has spread from Canada's larger metropolitan areas to smaller cities and towns.
Sustained abstinence is encouraged by reducing contact with those who are still using drugs. Thus, for the ex-alcoholic, avoiding his old 'drinking buddies' contributes significantly to continued sobriety. It has often been said that association with users is one of the most important factors in relapse into opiate dependence.'" In order to avoid the temptation to use once more, those attempting to stay away from heroin—or speed—must no longer communicate with many former associates and, in some cases, life-long friends. New relationships must be established with 'straight' people, many of whom, if not scornful of heroin or speed users, may be insensitive to the problems they face.255
The ability to find satisfactory employment seems to discourage relapse to dependent drug use.31, 252, 268 However, many 'ex-addicts' have severe impediments to successfully competing in the job market. For example, heroin use often begins during adolescence when the individual has not yet established stable social or economic relationships. In many cases, early termination of schooling and delinquent behaviour precedes drug use, thus delimiting future occupational opportunities. Once heroin dependence develops, the individual will begin to devote his energies to obtaining increasing amounts of money to support his habit, avoiding the police, and other activities which preclude working toward traditional goals through the educational and occupational structures. After years of 'hustling', it is understandable that many heroin dependents have few skills and little experience which could lead to lucrative or interesting legitimate employment.
Those who do manage to obtain and hold a regular job have a better chance of leaving the life of heroin behind.* 10 This factor seems to be most important for male heroin users who do not have the socially acceptable alternative of becoming a 'housewife', and must therefore find their 'ex-addict' identity in some sort of activity outside the household. But in addition to the problems posed by insufficient work records and low academic achievement, many former opiate dependents find prospective employers unwilling to hire people with criminal records, especially ex-heroin users.252 Many alcoholics, on the other hand, manage to maintain some form of stable career pattern in spite of their drug use and may, indeed, be impelled into treatment by concerned employers. Those whose work record is poor, however, will find difficulty in obtaining a job which is rewarding enough to help keep them away from alcohol. Unlike heroin users, however, they are unlikely to have the additional obstacle of a criminal record to impede their chances.
The patterns of drug use of a wife or husband and overall marital or familial stability play a role in encouraging abstinence. If both partners in a marriage are alcoholics or heavy drinkers, the prognosis for successful abstinence is poor as termination of use depends on their mutual efforts to attain sobriety. Heroin dependents often marry or live in common-law relationships with one another, and the same kind of co-operation is required to ensure that relapse will not occur. Permanent abstinence from heroin use sometimes stems from establishing a meaningul relationship with a non-user, although relapse may come later if the liaison fails.
The family of the alcoholic plays a significant role in either helping him to stay sober or propelling him into further drinking bouts. In recent years, agencies dealing with the rehabilitation of the alcoholic have come to realize that treatment is most effective when the family is involved.'23. 206 After years of drinking and unsuccessful attempts to stay sober, the alcoholic may find that his family, who learned to function without him and not to count on his participation in family affairs, may be unable to reinstate him in the household and trust him with important responsibilities.," Successful abstinence may hinge on the ability of the family to "forgive and forget" and, thereby, encourage satisfactory domestic reorganization.
Periods of abstinence from heroin use may be prompted by feelings of responsibility to family members, especially children.112 Similar sentiments may also precipitate attempts to quit smoking, particularly if a parent believes in the dangers of tobacco use and in the possibility that his children may follow his example.
Speed freaks are usually unmarried and rarely have children, but their parental family, if intact and willing to offer supportive assistance, can play a significant role in helping the speeder to remain abstinent. Unfortunately, many speeders come from broken homes and few express sufficiently positive attitudes toward or trust in their families to indicate a willingness to return to their parental homes.
A rewarding home and family life, the establishment of meaningful interpersonal relationships with non-users, and finding satisfactory employment are possible alternatives to a life of drug dependence; but some users turn to a pharmacological substitute. Alcoholics may switch to barbiturates or, conversely, barbiturate dependents may drink heavily when they lose access to their prescription drugs.33 Barbiturates may be used, alone or with alcohol, by abstinent heroin users, although they are usually considered to be poor substitutes.7°, 106 Many former heroin users drink alcohol to excess,* especially during the first year of abstinence, and a large proportion become alco-
holic.232, 253, 267
In some cases, abstinence will be initiated or sustained for personal reasons or because of chance factors. In one case, a fifty-pound weight gain was the reason given for not returning to heroin.263 Another individual was motivated to stop after his daughter was killed in a fire which he accidentally started while under the influence of heroin.232 For others, a number of extraneous events, such as blindness and arthritic paralysis, prevented continuation of a career of opiate use.33
There are several factors which have been hypothesized to affect abstinence rates among heroin users that have not been clearly borne out in research. The severity of the habit, ethnic background, criminal involvement, alcoholism and family histories of dependence have not been found to be related to successful abstinence.149, 252, 263
In recent years, especially since the use of methadone maintenance therapy has become popular, a number of heroin treatment facilities, using a variety of modalities, have become available in Canada (see Treatment Report). Heroin users may voluntarily apply for treatment for a variety of reasons, although what they expect of the agency may be quite different from what the agency expects to do for them.79 When the price of heroin on the street rises during periodic shortages, users may apply for withdrawal treatment or methadone maintenance, in order to avoid 'cold turkey' withdrawal, until favourable market conditions are re-established. Those whose hustling skills are minimal are most likely to respond to a 'street panic' in this way. Others may apply for treatment because of pressure from family or friends, with no real intention of becoming permanently abstinent. Some patients appear for methadone maintenance in the hopes that methadone will enable them to use less heroin and therefore reduce the cost of their drug use. Similarly, some heroin users ask to be withdrawn, not with the intention of remaining abstinent, but in order to reduce the per diem cost of their habits when they return to the street. Because of this disparity between the goals of treatment agencies and the intentions or expectations of the users themselves, some observers have recommended that patients should play an active role in determining the goals of treatment."
It appears that the various alcoholism treatment modalities and services are differentially available to alcohol dependents according to their wealth and position as well as the degree to which alcohol has disrupted their lives. The indigent 'skid row bum' is likely to become caught up in 'the revolving door syndrome' involving periodic arrests and incarcerations (see Treatment Report). Although he may be contacted by social workers or religious organizations and channelled into some form of treatment, his life alternatives are usually few and, seeing little to gain from continued sobriety, he is likely to return to his old environment and drinking patterns.
More financially fortunate alcoholics, on the other hand, are likely to be impelled into treatment by impending family or occupational disorganization. The lower- or middle-class drinker may turn to the well-publicized Alcoholics Anonymous or other foundations or public agencies which can offer inexpensive treatment. The well-to-do alcoholic, like the medical professional who becomes dependent on opiate narcotics, may receive treatment in an expensive, but discrete, private hospital or clinic. Industries are becoming increasingly aware of alcohol problems among their employees, and a number of programs have been established to attempt to help the alcoholic worker.
Although most tobacco smokers will make an attempt to stop on their own, perhaps adopting one of a number of popular 'systems' to reduce or terminate their consumption, in recent years smoking control clinics have been established to treat tobacco dependence.5 Statistics on abstinence and relapse patterns after such treatment are scanty, but it is evident that, like alcohol and heroin dependence, a pattern of heavy tobacco use is difficult to break and relapse may occur even after years of successful abstinence.
Insofar as the correctional system has a 'rehabilitative' component in that it demands abstinence from most drugs,* incarceration can be seen as a form of involuntary treatment. Among alcohol dependents, the 'skid row bum' is most likely to be arrested and jailed for at least as long as it takes him to 'dry out'. More financially fortunate alcoholics are unlikely to come to the attention of law enforcement officers unless arrested for public drunkenness, violent acts under the influence of alcohol, driving violations or other alcohol-related offences. As these offences are also committed by nonalcoholic drinkers, they rarely lead directly to any form of alcoholism treatment.
Most daily heroin users, on the other hand, have a high likelihood of being arrested—either for drug-related activities or offences committed in order to obtain money to buy heroin. Multiple convictions and prison terms are often expected by those deeply involved in the life of illicit opiate use, and jail is considered by many to be a 'part of living', or a 'lousy vacation place from your habit'.201, 232, 255 One would expect, therefore, that there is a better opportunity for therapeutic intervention in the institutional setting for heroin users than for those dependent on other substances, if indeed, effective treatment programs could be developed within that setting.
In the past, heroin users did not usually receive any special treatment in North American prison systems. However, in recent years, specific treatment programs for opiate dependents have been instituted in penal settings in both the United States and Canada. These programs are discussed elsewhere in this report (see Appendix I Treatment of Opiate Dependents in Federal Penitentiaries in Canada and Appendix L Civil Commitment in California).
An analysis of follow-up studies of drug dependents suggests that the proportion of people who are 'cured' and achieve a stable drug-free state after treatment or prison may not be much different from the proportion of individuals who become abstinent without professional or paraprofessional assistance, that is, those who 'mature out' on their own. In a ten-year follow-up study of heroin dependents who were incarcerated in Oakalla prison in British Columbia, it was discovered that only five to eight per cent of those who had made contact with the Narcotic Addiction Foundation in Vancouver were presumed to be abstinent, whereas 34 per cent of those with no contact had achieved this end.2'1, 213 This does not necessarily mean that the agency itself encouraged relapse, for those who did not appear for treatment, although they were similar to those who did on a number of significant variables, may well have been more marginally dependent or less involved in opiate narcotics use.
In some cases, it appears that abstinence becomes easier to sustain as a dependent person grows older. This process is usually referred to as 'maturing out', and although the concept was originally developed to describe cessation of opiate dependence, it has since been applied to other kinds of drug use. While success rates of tobacco-smoking clinics seem to be around 20 per cent, probably 15 per cent of regular smokers, including those not as highly motivated to quit as clinic patients, eventually stop using without treatment.224 Accumulating evidence suggests that alcoholism may be a self-limiting condition for some proportion of alcoholics and reduced intake, a change to non-problem patterns of use or total abstinence may occur without benefit of formal treatment in up to 25 per cent of the using population.38• 178, 214
The concept of maturing out of heroin dependence, although previously postulated by Scher,232 was popularized by Winick276 who concluded from his analysis of the records of the United States Federal Bureau of Narcotics (now the Bureau of Narcotics and Dangerous Drugs) that heroin dependence was a self-limiting process for perhaps two-thirds of the dependent population. There are a great number of problems with Winick's study, most of which centre around the U.S. agency's tabulating procedures.* Some of the persons that Winick assumed to have matured out may have been dead or in prison; others may have become 'hidden addicts' insofar as they acquired the skill or resources to avoid encounters with law enforcement agencies. Henderson suggests that Winick's sample may not have been representative of even the known heroin-using population and that a significant proportion may have been only marginally dependent.117
Although Winick's data do not satisfactorily support his theory,268, 269 maturing out does occur in a proportion of cases according to other studies. It appears that age is correlated with the frequency and duration of abstinence periods among heroin dependents,77, 122, 213, 264 although Waldorf suggests that the number of years of heroin use is a stronger predictor of long-term voluntary abstinence than is age.t 268, 269 Vaillant found two out of five subjects in their forties to have accomplished stable abstinence, although a similar proportion were dead or institutionalized. 265 Similarly, there is a higher probability that tobacco smokers over 30 will be successful in abstaining from this drug, and this probability rises with increasing age. The average daily consumption of cigarettes tends to decline in middle age. 65. 224 Cahalan's follow-up of a national sample of U.S. drinkers reveals that drinking problems decreased with age, with a sharp drop at the age of 50 and another after age 70 for men. He found few women with drinking problems after the age of 50."
`Spontaneous' recovery from problem levels of alcohol use is most likely to occur when the drinker becomes fully aware of the extent to which alcohol is causing progressive dissolution in his life situation.'" Alcoholics are said to reach their lowest point in their own eyes as well as in the opinion of their friends and family in their late thirties.62 Cahalan and his associates concluded that lower levels of drinking among older people are probably attributable to voluntary cessation or decrease in alcohol consumption rather than generational or cohort differences in alcohol use."
Although tobacco smoking has no effects comparable to alcohol on the life style and self-conception of the user, it is reasonable to assume that fear of the harmful physical effects of tobacco use, particularly on a body weakened by advancing age, must play some role in the decision to terminate use, particularly if cessation of tobacco use has been recommended by a physician.
Although there are no systematic data on the cessation of chronic meth-amphetamine use, it appears that many speed freaks voluntarily refrain from further intravenous consumption of this drug after a year or two of sustained use. In many cases, the physical and psychological demands of the drug, coupled with increasing reflection on these problems and the viability of alternative life styles, are responsible for the decision to abstain.103 However, the relative newness of this phenomenon renders it difficult to generalize about the reasons for cessation of speed use or the chances of successful abstinence.
There is no question that, for some, a life style of heroin dependence becomes unbearable after a period of time, especially among those whose ability to support their habits has declined to such a point that even other users no longer have respect for them.269 Women tend to disappear from the known dependent population around the time that a career as a prostitute would be coming to an end, that is to say, in their late thirties and early forties.112, 117 That the way of life of the heroin user on the street, in jails and in treatment facilities should become prohibitively demanding in later years is not surprising; what is more remarkable is that some individuals manage to survive and stay actively dependent, even after decades of heroin dependence.
It is evident that there are a number of variables which affect abstinence and relapse patterns. 'Spontaneous' loss of craving for a drug, although it may conceivably occur in some cases, is probably mediated through one or more of the economic and social conditions we have described above. Maturing out is most often a complex phenomenon and should be understood as such. Abstinence, even for prolonged periods, usually does not imply loss of desire for the drug of dependence, and craving often continues for the lifetime of those who are ostensibly 'cured' of their dependence.*33
Termination of dependent alcohol, methamphetamine, or heroin use usually represents a desire to seek out a new value system and a different way of life. As Vaillant suggests, relapse to heroin use may be more due to a poverty of life alternatives than to the extent to which the drug may appear to have answered the needs of the individual. C7 The struggle against relapse begins immediately after detoxification when the individual begins his attempt to become an 'ex-' or 'non-addict', and to re-order his life style and his relations with others.
The response of relatives, friends and employers to those who are trying to stop using dependence-producing drugs is crucial, not only to their success in this endeavour, but also to the likelihood that they will be able to take on the identity of a 'normal' person. Heroin relapse often occurs when obstacles to this process necessitate a re-definition of self as a junkie'.208 Similarly, the reformed alcoholic, although not faced with the additional problem of becoming an 'ex-criminal' as well as an 'ex-addict', must constantly reaffirm his self-image as a responsible and self-controlled abstainer.f
Life is bitter and the prognosis is poor for most heroin dependents and alcoholics. Although the daily life of tobacco smokers is not radically affected by their use of nicotine, it may well be shortened, and their attempts to cast off this dependence do not appear to have met with dramatic rates of success. However, the termination of non-dependent use or the use of nondependency-producing drugs does not engender the host of problems faced by chronic users of opiates, alcohol, tobacco, or methamphetamine, and, consequently, is much easier to accomplish.
* Dai, in his study of opiate dependency in Chicago, reached the same conclusion more than 35 years ago when he noted that the "... process in which this pattern of opium addiction is taken over by an individual is not very much different from that in which other cultural patterns are transmitted"?'
* There are a relatively small number of persons whose initial drug use was unwitting rather than volitional. This category primarily includes non-medical drug users whose first use of their drug was under medical auspices or whose initial drug experience was accidental in the sense that they were unaware of the psychotropic properties of the substance they were ingesting. Individuals who first received opiates in the course of normal medical practice for the relief of pain and whose consequent dependence has been maintained despite the cessation of the medical condition that initially prompted such use, exemplify this first situation; while instances of unsuspecting persons being given LSD or other hallucinogens (as documented in the case of the 1966 Los Angeles 'Acid Test'7°) illustrate the second of these rare initiation processes.
* The relationship between various types of drug use is extensivly considered elsewhere in this appendix. (See Annex 1 to this appendix and "Patterns of Multiple Drug Use" on page 726.) It should be noted, however, that both the opportunity and desire to try a personally 'new' drug are somewhat a function of one's appreciation of previous drug experiences and the extent of one's involvement in the world of drugs. First use of hallucinogens, for example, is almost always preceded by a period of 'successful' cannabis experimentation: the more extensive the use of cannabis, the greater the probability of hallucinogen
use 176, 227, 243
1' Dependent persons do occasionally play an important role in introducing heroin use to others. The most typical of these situations is a love relationship, marriage or common-law union in which the non-using partner first tries heroin in order to experience their dependent spouse's or lover's drug of choice. A large proportion of female addicts were first introduced to heroin in a relationship of this nature.78. 128. 172.
* The obviousness or subtlety of a drug's effect is a function of various factors, including the drug itself, the mode of administration, the 'set' and 'setting' of the using situation, and the dosage consumed. The psychotropic effects of small doses of cannabis, cocaine or a sedative, for example, may be 'missed' by a naive user, while an injection of heroin or methamphetamine will have immediate, profound and unignorable consequences.
* It could be argued that hallucinogen use which is oriented to self-improvement and awareness is actually a form of functional drug use.
* Comprehensive discussions of various 'progression' theories may be found in several papers by Erich Goode2" as well as the published and unpublished works of Jerry Mandel?", "T,
* Some observers have tried to see if this hypothesis of a constant proportion of cannabis users later becoming heroin users is reflected in arrest statistics. The relationship between the arrest rates for cannabis and heroin have been used as a basis for both 'pro-progression' and 'anti-progression' arguments.", "7.181, 158, 158 There are, however, major methodological problems involved in the use of this kind of indirect indicator. In the first place, heroin users are believed to be more vulnerable to arrest than cannabis users, and therefore heroin arrestees would represent a larger proportion of the real using population. In addition, heroin users are likely to experience multiple arrests, thus inflating their numbers.4° Finally, it is generally believed that arrest data are most often reflective of law enforcement activity and emphasis than of incidence of use in the population (see C. 1 Introduction above).
Another approach that has been utilized is to search the records of heroin users to see if they were previously cannabis (or other drug) users. C. Hammond, late of the Division of Narcotic Control (now, the Bureau of Dangerous Drugs), supplied the Commission with statistics on those cases which came to the attention of this agency between January 1969 and October 1970. Although this data suggest what proportion of known Canadian heroin users were known to also have used cannabis, it fails to reveal what proportion of the cannabis-using population is likely to subsequently use or become dependent on opiate narcotics.
* Cases have also been reported of older brothers introducing cannabis to their younger brothers in an attempt to provide what they see as a less harmful substitute for glue or other solvents."
* See Appendix A.5 Hallucinogens and Their Effects for a discussion of LSD and chromosome damage.
* The prognosis for sustained abstinence from heroin is generally better for people who become involved with heroin after the age of 25, and undoubtedly the intervening variable in many of these cases in some sort of stable employment prior to becoming dependent.'"''
* O'Donnell reports one case of successful heroin abstinence which led to compulsive eating.lm Some people who try to quit smoking also complain of increased food consumption and weight gain.
* Since tobacco is the only drug sanctioned for non-medical use in prisons and is thus an important form of currency as well as a diversion from the prison routine, it would appear that, if anything, incarceration encourages increased use of nicotine.
* At the time of Winick's study, the Bureau of Narcotics and Dangerous Drugs had not described its data collection procedures in sufficient detail to evaluate the accuracy of its figures. Apparently no uniform instructions were given to the reporting agencies, and Linde-smith, after analysing the Bureau's register, concluded that the enterprise as a whole appeared to be more of a public relations effort than a serious attempt at enumeration.15° Other studies, however, do not support this contention.242
* Some drug dependents do not achieve permanent abstinence until medical complications or death interrupt their drug-using careers. The mechanisms by which this occurs are discussed in detail in another appendix (see Appendix A The Drugs and Their Effects).
f Ex-smokers are often accused of over-enthusiasm in this regard, regaling their friends—especially those who have been less successful in their attempts to quit—with detailed analyses of their smoking careers and the precise period of time which has elapsed since their last cigarette.