| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 161 |
| Yesterday: | 251 |
| This Week: | 161 |
| Last Week: | 2221 |
| This Month: | 4749 |
| Last Month: | 6796 |
| Total: | 129348 |
| - |
Drug Abuse
C.2 EXTENT OF USE
From the point of view of the individual consumer, the non-medical use of any given drug occurs within a context of multiple drug use, including both the medical and non-medical use of drugs, and the use of substances that an individual may not regard as drugs, such as alcohol, tobacco or coffee. In this section we examine the extent of use of individual drugs and, in the next section, present summary data on the social characteristics of Canadian drug users. Finally, we discuss patterns of drug use and the multi-drug use context. This latter discussion is complemented by Annex 1 to this appendixv in which quantitative data on the relationships between various drugs is analytically reviewed.
Research during the last four years has produced a respectable volume of data on the extent of drug use but these studies describe a patch-work quilt of populations. Certain groups, particularly adults and people in rural areas, are still largely ignored by drug researchers. Because of this fragmentation of the data, formal methods of extrapolating the extent of drug use in Canada are not appropriate. The "estimates" that follow are sound impressions rather than firm estimates, but we feel that they give the best sense of the available information, and that they are near enough to the present reality of drug use in Canada to be useful.
OPIATE NARCOTICS
`Opiate narcotics' or 'opiates' in this context will refer to opium and its natural alkaloids and related synthetic compounds, including heroin and methadone. (See Appendix A.2 Opiate Narcotics and Their Effects.)
Many of those in drug-using circles who state that they have used `opiates' are probably referring to opium preparations other than heroin including, in some cases, codeine-containing pills or cough syrups. They may also be referring, incorrectly, to `opiated' hashish, an apparently mythical substance, the existence of which has never been documented in Canadian street-drugs analysis programs. With regard to patterns of use, opium is occasionally used, when available, in a manner similar to cannabis smoking. Heroin, on the other hand, suggests to youthful drug users a much more serious and dangerous drug. It is unfortunate that so many studies simply ask exclusively about 'opiates', and do not seek data that would allow us to empirically distinguish between the use of heroin and the use of other opiate narcotic drugs. Furthermore, heroin use does not necessarily imply intravenous use of the drug; experimental users, in particular, tend to use inhalation as their primary mode of consumption.
In the following pages, we will attempt to estimate the number of heroin and methadone dependent persons in Canada. Information on the extent of opiate use other than heroin or methadone is, unfortunately, scanty.
The number of "known habitual illicit narcotic drug users" (hereafter referred to as "habitual narcotics users") recorded by the Bureau of Dangerous Drugs (B.D.D.) of the Department of National Health and Welfare is shown in Table C.1. Table C.2 indicates the changes in these numbers from year to year. The number of known habitual narcotics users was relatively stable in Canada from 1962 to 1969, and showed marked increases in 1970, 1971 and 1972.
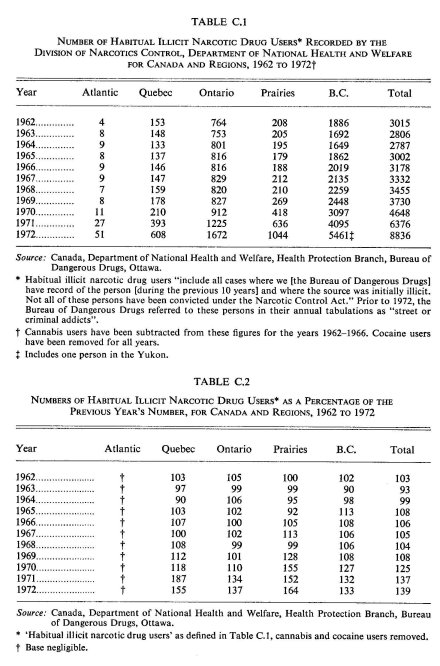
Opiate users are added to this B.D.D. list if they come to the attention of the police, or if they are prescribed methadone for the treatment of dependence. They are dropped from the list if they are not heard of in ten years. There are, therefore, two sources of error in the list. First, not all habitual narcotics users come to the attention of the police or the Bureau of Dangerous Drugs, and, of those who do, there is usually a considerable timelag between first contact with opiates and becoming 'known' to the B.D.D. Second, not all of those on the list are necessarily dependent on opiates. A small number are users of cocaine, and a larger number, about five per cent in 1971, were cited as using 'unknown substances'. Since patterns of cocaine use differ considerably from heroin or methadone patterns, we have removed cocaine users from the B.D.D.'s habitual narcotics users figures. For similar reasons, cannabis users (who were recorded by the B.D.D. until 1966) have also been removed. Not all of those who are arrested for a heroin-related offence (particularly a possessional or importing offence) are necessarily dependent, but their names will still be added to the list. In addition, a certain proportion of those on the list will have died, left the country, or their dependence will have remitted in the decade before their names are automatically removed from the list. Thus, not all persons in the known habitual narcotics users files are necessarily dependent on opiates, and not all of those who are dependent are listed as 'known'.
Some additional comments are in order on the significance of these figures. They are used here as an indicator of the number of opiate-dependent persons in Canada. It is generally believed that these figures represent an underestimate of the total number of dependents in the country, but it is usually assumed that when the number of known habitual narcotics users rises it has done so because of an increase in the heroin-dependent population at large and, thus, may be considered to be rising more or less in proportion to this general increase. As indicators, these figures belong to the indirect type of measure discussed in C.1 Introduction above, and, as such, are subject to varying interpretations.
If the true number of dependent persons in Canada is a constant function of the number known to the B.D.D., we may still use these figures as an estimate of the actual number of users. However, there is reason to believe that this is no longer the case as the B.D.D. is, apparently, presently collecting some of these names through different channels than it did in the past. The so-called 'new addict' is said to be younger and, unlike traditional heroin dependents, appears for treatment (particularly methadone maintenance) after only a few months or years of use.53 In the past few years, we have seen an increasing proportion of new names which have been gathered by "retail reports", that is, primarily through methadone maintenance prescriptions.'" The sudden upsurge in the number of recorded habitual narcotics users in 1970, 1971 and 1972 could, then, reflect the increasing popularity of methadone maintenance as well as the tendency for young users to appear early for treatment.
Nonetheless, a growing number of new names have also been derived from police reports. If, indeed, these new names represent new, young users, it is not unreasonable to assume that many of them reflect changes in law enforcement activity during the past few years. With the rise in cannabis and hallucinogen use, law enforcement officials have become much more aware of youthful drug use, thus increasing the probability that a young person or his residence will be searched. In addition, drug squads across the country have recently been concentrating on 'hard' drugs, shifting from their earlier focus on cannabis and LSD. Thus, it seems a greater number of opiate users are appearing on the lists of the Bureau of Dangerous Drugs, but we cannot be certain that this increase is proportional to the true increase in use of the population at large.
A study by Oki of Toronto heroin users known to the Addiction Research Foundation of Ontario, the R.C.M. Police, or the Bureau of Dangerous Drugs, indicated that 64 per cent of the combined total were known to the B.D.D.186 If this proportion holds for all of Canada, there were roughly 10,000 heroin users in Canada in 1971 and 14,000 in 1972 who were likely to be known to some data-gathering agency. However, it must be remembered that heroin users are more likely to be known to treatment personnel in large urban centres like Toronto and Vancouver where treatment programs are readily available. Furthermore, this estimate excludes all those users who were not known because they had not yet come into contact with law enforcement officials or had not sought treatment.
A preliminary Commission analysis of heroin- and methadone-related deaths in Canada from 1970 to early 1972 revealed that a little over 50% of the dead had been unknown to the Bureau of Dangerous Drugs as opiate narcotic users. These data imply that the number of habitual opiate narcotics users known to the B.D.D. in 1970-71 represented only about one-half of the actual opiate-using population (which suggests an estimate of almost 13,000 such users in 1971). We do not have adequate information for 1972, but we suspect that the proportion of opiate narcotics users known to B.D.D. may have recently changed as a result of the expansion of their information acquisition network, changes in patterns of drug use and other factors.
When the Commission conducted its field studies in May 1972, it received high and low estimates from "knowledgeable persons" in major cities of Canada as to the numbers of daily users of heroin and methadone.'" These estimates are highly impressionistic, even though they represent some of the best informed opinions in the cities which were surveyed. High and low estimates were made for the major regions of Canada, and the result was a low daily user estimate for the country as a whole of 7,525 and a high of 14,800. The R.C.M. Police, on the other hand, have estimated that in the fall of 1972 there were between 12,400 and 14,410 'heroin addicts' in the country, and although their regional breakdown differed somewhat from that derived from our survey of knowledgeable persons, the high totals are not significantly different.
Because of the relative 'invisibility' of occasional users, our field workers' estimates of the size of this population are even less reliable, but suggest numbers in the 15,000 to 30,000 range for the year 1972. Smart, Fejer and White242 found that 4 per cent of Toronto high school students reported use of opiates in the six months prior to their 1972 survey, and that 1.9 per cent (some or all of whom may have answered the 'opiates' question affirmatively) claimed to have used heroin during the same period of time.
While there is no reason to doubt the findings of this Toronto survey, it would be unwise to project these figures to the country as a whole as Vancouver is probably the only other Canadian city with comparable heroin availability. However, based on what little is known about the relationship between opiate-dependent and non-dependent using populations, it is not unreasonable to assume that in 1972 Canada's approximately 15,000 daily heroin and methadone users were complemented by an additional 50,000 occasional users of these drugs. An unkown proportion of this latter group is, of course, at risk to dependence.
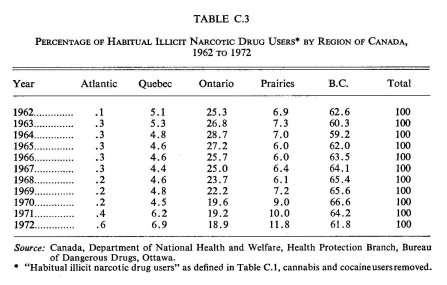
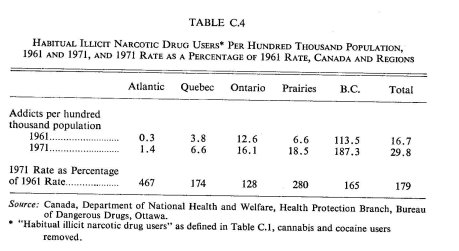
Heroin dependence has been concentrated in British Columbia for many years. Tables C.3 and C.4 indicate that the proportional rate of increase in habitual narcotics users on the lists of the Bureau of Dangerous Drugs between 1961 and 1972 is highest for the regions with the smallest proportions of known users, particularly the Atlantic region and the Prairies.
The Commission's field studies of May 1972 indicate that methadone use resulting from careless prescribing by physicians in Halifax accounted for most of the increase in opiate use in the Atlantic region.104 Montreal has witnessed a similar phenomenon. There has been an increase in heroin use in Ontario, primarily in the populations traditionally associated with its use, and mainly along the Toronto-Windsor axis where there is a good deal of contact between American and Canadian drug users. In the west, British Columbia has experienced an increase in heroin use, and more particularly in occasional (and not necssarily intravenous) heroin use among young people. British Columbian heroin-using patterns tend to diffuse to Alberta, where, in the past five years, there has been a marked increase in the number of known opiate users: from 123 in 1968 to 614 in 1972.46 The extent of heroin use in Saskatchewan and Manitoba has also increased, but not as dramatically as is the case with Alberta.1" Provincial patterns of heroin distribution are presented in Appendix B.2 Sources and Distribution of Opiate Narcotics.
There is a consensus among Canadian observers that opiate use is increasing, but no one claims to know the rate of increase. As well, no authority feels able to predict when the increase in heroin use will peak or reach a stable plateau, if ever. One United States researcher, John Newmeyer of the Haight-Ashbury Free Medical Clinic, on the basis of a survey of drug-dependent young people in San Francisco, suggests that a plateau has been reached there, and believes that use will peak throughout the United States by 1974.182. 183 The random samples of identifiable populations available for Canada have not permitted any broad generalizations about whether or not this possibility applies to this country as well.
AMPHETAMINES AND AMPHETAMINE-LIKE DRUGS
We are concerned here with 'pep pills', 'diet pills' and 'speed'. These are preparations of amphetamine, dextroamphetamine, or methamphetamine (the last of these being the drug of choice of 'speed freaks'), and the amphetamine-like drugs such as phenmetrazine and methylphenidate. The critical distinction for our purposes is not the particular chemical used but, rather, the dose level, frequency of use, and whether it is taken orally or intravenously. The physical, psychological and social concomitants of these different using patterns are reviewed elsewhere in this report; a discussion of the extent of both oral and intravenous types of use follows.
INTRAVENOUS SPEED USE
The intravenous use of speed (methamphetamine) is commonly associated with the 'speed freak' phenomenon, but may occur in other drug-using subcultures as well. The term 'speed freak' denotes not only the use of a substance (speed), but also the level-of-use (chronic high-dose use) and the mode of administration (intravenous). No survey of a Canadian population has asked its respondents whether or not they are speed freaks. Rather, they survey, in order of increasing specificity, whether they have used 'stimulants', `amphetamines', 'speed', or `methedrine' (methamphetamine). A few ask for the mode of administration. Published results, therefore, often do not allow us to distinguish speed freaks from others who may occasionally use speed intravenously, or intravenous users from oral users. Both the Commission's national survey of high school students and the Narcotic Addiction Foundation of British Columbia's study of Vancouver high school students 18° indicate that a fraction of amphetamine users in those populations have used speed intravenously, but most of these probably used only on an experimental basis.
The numbers of chronic, regular, high-dose, intravenous amphetamine users probably reached its peak in the summer of 1970. All told, based on participant-observation studies and interviews with knowledgeable persons in Canada's major cities, we estimate that there were between 2,000 and 3,000 such individuals at that time, concentrated very largely in the centres of Toronto, Montreal and Halifax. There were perhaps another 3,500 to 4,500 who used high doses intravenously, but not on a regular basis. By the summer of 1971 the numbers in the centres of all of these cities combined fell to perhaps not much more than 1,000 to 1,500 persons. But intravenous users of speed, particularly those involved in intermittent patterns of use, had increased markedly in the suburbs of these cities and in a number of smaller cities in southern Ontario, western Quebec and the Maritimes.103
In the summer of 1970, many intravenous amphetamine users used the drug on a regular basis—several injections a day for up to two weeks at a time with only a few days between such 'runs' (see C.4 Patterns of Use). This is still the pattern for a much smaller proportion of the total intravenous amphetamine-using population. In addition, however, there now appears to be a population of high-dose, intravenous users who take the drug for only brief periods of time, on weekends or on an episodic basis. If the totals of both these types of users are combined we would estimate that the number of high-dose users was about the same in the summer of 1972 as it was two years earlier, or perhaps marginally larger. Because very few persons regularly use speed for more than a couple of years (see C.4 Patterns of Use), there is a continually high rate of withdrawal from the intravenous speed-using population which limits the growth of this phenomenon to the difference between new recruits and new abstainers. This difference is presently such that Canada's speed-using community appears to be more or less numerically stable, although it is a much more dispersed population than was the case two or three years ago.
ORAL USE OF AMPHETAMINES AND AMPHETAMINE-LIKE DRUGS
While Canada's speed freak population appears to have numerically stabilized, the oral use of amphetamines and amphetamine-like drugs has continued to grow. There has doubtless been a degree of 'pill popping' for functional purposes for many years among such people as waiters and waitresses, athletes, students, business executives and entertainers. This phenomenon was still increasing at the time of the new amphetamine regulations of January 1, 1973. Reports from some regions suggest that some tavern-goers, particularly younger ones, have established a pattern of consuming oral amphetamines or amphetamine-like drugs together with alcohol. Reports from all regions indicate that oral use of these drugs is particularly popular among university students, especially during exam periods.'"
Surveys of Canadian populations, primarily involving high school samples, that have asked about any amphetamine or stimulant use (the level-ofuse being defined in almost all cases as any in the last six months) have found prevalence of use rates that are remarkably uniform (ranging from five to nine per cent) and that show no sign of significant change from 1968 to 1972.6, 17, 32, 34, 42, 78, 80, 81, 82, 108, 114, 115, 154, 180, 205, 225, 240, 241, 251, 258, 272, 273 The Commission-sponsored surveys, conducted in the spring of 1970, found the non-medical use of 'pep pills' reported by three per cent of high school students, six per cent of college and university students and three per cent of the national adult sample. 'Diet pills' had been used non-medically by one per cent of the high school and adult samples, and by three per cent of the college and university sample. 'Oral speed' use was reported by three per cent of high school and less than one per cent of college and university students. Combining the high school use rates reported by the Commission surveys allows us to suggest a representative figure for the prevalence of nonmedical use of any amphetamine or amphetamine-like drugs in Canadian high schools of seven per cent. Josephson, et al., in their May 1971 national survey of American youth aged 12 to 17, found that nine per cent had used amphetamines at some time, which tends to support our estimate for Canada.128 Between 15 per cent and 20 per cent of the high school students who use amphetamines or amphetamine-like drugs (generally defined as 'pep pills' or 'diet pills') use them more than once a month.143, 243
The Commission's national survey indicates that four per cent of Canadian adults at some time orally used amphetamines or amphetamine-like drugs non-medically. The one other random survey of Canadian adult use of psychoactive substances, that of Fejer and Smart, indicates roughly similar results: as of the spring of 1971, four per cent of Toronto adults had used "stimulants" medically or non-medically during the previous 12 months.82 We note later that only ten per cent of Toronto adult users of barbiturates or tranquilizers obtained them without a prescription. By contrast, more than a third of the stimulant users in this same study obtained these drugs without a prescription.
Among adult "stimulant" users, Fejer and Smart found that 51 per cent of their Toronto sample used these drugs daily, seven per cent used them between two and five times per week, and about 19 per cent used them between once a week and once a month." Thus, 77 per cent of those Toronto adults who used stimulants (whether medically or non-medically) did so at least once a month. The Commission's national adult survey found that an almost identical proportion of those respondents using 'diet pills' or 'pep pills' at the time of the study did so once a month or more.
If we accept the Commission and Toronto survey findings regarding the incidence of adult use of amphetamines and amphetamine-like drugs (i.e., about four per cent), and if we assume that about one-third use these stimulants without benefit of prescription at least some of the time, then we would estimate that 1.3 per cent of Canadians 18 years of age and over have used stimulants non-medically in the past year, or approximately 171,000 persons. If we apply the high school estimate of seven per cent to Canadian youth, we have 182,000 users, for a total of 353,000 Canadian users of amphetamines and amphetamine-like drugs for non-medical purposes in the past twelve months. The majority of this use would be of the occasional or experimental variety.
CAFFEINE
Caffeine and related xanthines, in the form of coffee, tea, cocoa and cola drinks and various over-the-counter preparations (for example, No Doz®), is the most commonly used stimulant in Canada. Canadians drink 33 million cups of coffee and 30 million cups of tea every day. Canada's tea consumption is only one-quarter that of the United Kingdom or Ireland on a per capita basis, but it is three times that of the United States.281 Canada's per capita coffee consumption is slightly below that of the United States.
The Pan-American Coffee Bureau surveys coffee consumption in Canada for an 'average winter's day' when use is presumably at a maximum, and the following statements are about use on such a day. The data are for 1970, but the phenomenon appears sufficiently stable to allow us to apply them to the present. Sixty-four per cent of Canadians ten years of age and over drank coffee on an 'average winter's day', drinking an average of three and one-tenth cups each. Complete data on levels-of-use are not available for Canada. In the United States, however, the 20 per cent of the population who used coffee most frequently each consumed an average of seven and one-half cups of coffee on this typical day. Fifty-three per cent of Canadians drank tea on an 'average winter's day'. We do not have adequate information to comment on the consumption of xanthine-containing cola and cocoa drinks.
HALLUCINOGENS
An impressive array of substances have hallucinogenic properties in greater or lesser degree, including certain varieties of morning-glory seeds, nutmeg, mandrake, belladonna, sweet flag, yage, a number of mushrooms, including the fly agaric, panaeolus, and psilocybe (the source of psilocybin), the peyote cactus (the source of mescaline), DMT, DET, DOM (STP), PCP, MDA, and, of course, LSD. Only the last three of these have any currency in the Canadian illicit drug market, and street samples alleged to contain more esoteric hallucinogens are almost always found, on analysis, to be PCP, MDA or LSD, or some combination of these drugs. Those who buy these substances have little control over or knowledge of the quality and purity of their purchases. Because of this uncertainty of identity, we will not attempt to distinguish among substances here. It should be remembered, however, that there is great variation in the potency of these materials, and that some unidentifiable proportion of use will involve low potency drugs or even inert substances that users will report as true hallucinogens. These problems are further discussed in Appendix A.5 Hallucinogens and Their Effects and Appendix B.5 Sources and Distribution of Hallucinogens.
Information derived from Commission field studies in May 1972 suggests that the number of current hallucinogen users has numerically stabilized, with as many people stopping use as beginning it.'" This is in accord with an observation made by Goode several years ago about hallucinogen use in the United States: ". . . probably more than any other drug in use the drop-off after the first experience is precipitous. There [is] typically little desire to continue beyond the experimental first few instances."'"
The Commission surveys (which are the only national surveys to ever have been conducted in Canada) indicate that by the spring of 1970, four per cent of high school students and eight per cent of university students had at some time used hallucinogens. Use in the adult population was only about 0.6 per cent. However, other Canadian surveys, primarily conducted in metropolitan areas, suggest that these figures understate use in 1970.6, 17, 34, 42, 81, 88,
108, 114, 115, 133, 154, 180, 205, 219, 225, 239, 240, 241, 242, 251, 258, 272, 273 These studies indicate a current incidence of use of five to ten per cent in high school populations, and over ten per cent in university populations. There was a dramatic increase in hallucinogen use between 1968 and 1970, with use doubling every year. We can assume that the rate of increase has been much slower from 1970 to 1972. Evidence from the United States, usually a bell-wether for North American drug use, supports this assumption. In a national survey of American college students, the proportion of students claiming to have ever used LSD rose from 11 per cent in 1970 to 13 per cent in 1971.197 Furthermore, a recent longitudinal survey conducted among Toronto high school students has found that the prevalence of LSD use in the previous six-month period declined from 8.5 to 6.4 per cent between 1970 and 1972, while use of "other hallucinogens" rose only slightly from 6.7 to 7.2 per cent during this same two-year period, thus indicating a relatively stable incidence of hallucinogen use.242 Nationally, there has probably been a slight increase from 1970 to 1972 in the proportion who have ever used hallucinogens. The proportion among high school aged youth across Canada who have ever used these drugs is probably not over ten per cent, and we will use that as a maximum estimate for persons between 12 and 17 years of age.
The Toronto adult survey indicates that 2.6 per cent of this population had used LSD in the twelve months preceding the spring of 1971.2"9 This figure is in line with that for New York State of a year earlier52 and with that for adults in two San Francisco Bay area communities surveyed in 1967 and 1969.159 It is likely, however, that adult hallucinogen use is higher in metropolitan than rural areas. It does not, therefore, seem appropriate to use the Toronto figure above as a norm for the entire Canadian population over 17 years of age. We have, rather, chosen a figure between the Commission survey's 0.6 per cent ever used rate and the Toronto study's 2.6 per cent current rate of use, namely 1.5 per cent, as a conservative estimate of the proportion of adults who have ever used hallucinogens. This estimate, combined with that for persons between 12 and 17, indicates that approximately 470,000 Canadians have at some time used hallucinogens, which is about three per cent of the Canadian population aged 12 and over. As indicated above, the number of current users appears to be stable.
It appears that hallucinogens are used more than once a month by about 15 to 25 per cent of the Canadian high school students who use these drugs.241, 242, 243 It is not possible, at present, to make a definite statement concerning the frequency of hallucinogen use among Canadian college students and adults because of the paucity of reliable level-of-use data about these populations.
ALCOHOL
Alcohol use is widespread in western society. Use has been increasing in Canada (and also in the United States), particularly among young adults and adolescents. This trend was observable even before the recent lowering of the legal drinking age throughout much of Canada.
Canadian surveys of local high school populations record alcohol consumption by anything from 40 to 87 per cent of students, despite the fact that such consumption is illegal for almost all of them.6, 17, 80, 81, 108, 115, 180, 219, 225, 240, 241, 242, 251, 272, 273 The Commission's high school survey, which provides the only national data, gives the lowest proportion of any Canadian high school survey for those who have ever drunk alcohol: only 33 per cent. Thirteen per cent of this sample, a little over one-third of all high school drinkers, had had a drink more often than once a month in the previous six months, as of the spring of 1970.
Surveys of university students in Canada and the United States yield estimates of between 80 and 97 per cent as having ever had a drink.17. 154. 198 The Commission's college and university survey found that 83 per cent of students reported ever having had a drink as of the spring of 1970, and that 59 per cent of the students claimed to have drunk more than once a month during the previous six months. The Commission's national adult survey indicates that 66 per cent of Canadian adults have had a drink at some time, with one in five Canadian adults (or 2,780,000 persons) claiming to drink alcohol more than once a week. De Lint, Schmidt, and Pernanen" found that, in 1969, 80 per cent of the Ontario population aged 15 and over, or 82 per cent of the Ontario population aged 20 and over, were alcohol drinkers.
Because the use of alcohol is increasing and because the legal drinking age has recently been reduced through much of the country, we feel that the national Commission survey findings of 66 per cent drinkers among Canadian adults and 33 per cent drinkers among Canadian adolescents are not reliable reflections of current alcohol-using rates in these populations. Instead, we will use a figure between the Commission's findings and those of the Ontario survey, namely 75 per cent, as an estimate of the prevalence of alcohol use among Canadians aged 18 and over, and an estimate of 50 per cent, which is likely conservative, for use among Canadian adolescents. These two estimates yield about 11,716,000 Canadians who have had a drink at some time. (The Addiction Research Foundation of Ontario' estimated that there were 11,612,000 alcohol drinkers over 14 years of age in Canada in 1969.) Approximately one in ten Canadian drinkers is drinking illegally because he is under age. It has been estimated that 5.31 per cent of Canada's drinking population (that is, about 617,000 persons) consumed a 'hazardous' amount of alcohol per day in 1969.' On the basis of liver cirrhosis mortality data, the Addiction Research Foundation of Ontario has estimated that there were 308,200 alcoholics in Canada in 1967, or about 2.8 per cent of all alcohol drinkers in that year.'
The de Lint, Schmidt and Pernanen" 1969 survey of Ontario drinking habits found that about 15 per cent of Ontario residents (or 19 per cent of Ontario's non-abstaining population) drank alcoholic beverages (in most cases beer) more frequently than twice a week. Daily alcohol drinkers accounted for less than six per cent of Ontario residents, or about seven per cent of all Ontario drinkers. Of those Ontario residents who drank alcohol in the week preceding their interview (71 per cent of the non-abstaining population), by far the majority (76 per cent) consumed less than 21 centiliters of absolute alcohol during that week (or less than three centiliters a day), while only about three per cent of this group (or less than two per cent of the total Ontario population over 14 years of age) consumed more than 70 centiliters of absolute alcohol during the surveyed week (or more than 10 centiliters of absolute alcohol per day).
BARBITURATES, MINOR TRANQUILIZERS AND OTHER SEDATIVE-HYPNOTICS
Here we are concerned with the barbiturates (such as Seconal® and Nembutal®), non-barbiturate sedative-hypnotics (such as Mandrax®), and the minor tranquilizers (for example, Librium® and Valium()). We omit the major tranquilizers as they are rarely employed for non-medical purposes. These preparations are known by a variety of names in the argot of drug users, but are generally classed together as 'downers' because of their sedating effects. Certain substances that could be treated under this heading are usually used for their hallucinogenic or inebriant, rather than sedating, qualities. Among these are alcohol (which was discussed above), Datura innoxia (thorn-apple), Datura stramonium (Jimson weed), and certain belladonna alkaloids such as scopolomine. These last three are only rarely used, and are omitted from this account for want of information.
The Commission's surveys suggest that about one-third of Canadian adults had taken 'sedatives' at some time by 1970, whether medically or non-medically, that about one-quarter had taken 'sleeping pills', and one-quarter `tranquilizers'. These three groups overlap to some extent. Current and frequent use is less common For each of these three substances, roughly one Canadian adult in 20 had used it more often than once a week in the previous six months, whether for medical or non-medical purposes.
About one-fifth of Canadian college and university students had used each of 'sedatives', 'sleeping pills' and 'tranquilizers' by 1970, while 15 per cent of high school students had used 'sedatives', and 11 per cent had used each of 'tranquilizers' and 'sleeping pills'. The proportions of current users in high schools and universities are lower than those of adult users of these drugs.
In December 1971, Sidney Cohen (head of the Center for the Study of Mind-Altering Drugs at the University of California, Los Angeles) predicted that 1972 would be the "year of the downer".235 Field studies conducted by the Commission in May 1972 suggest that this prediction may well have been a valid one. Our reports indicate that the non-medical use of barbiturates, as well as the non-barbiturate sedative-hypnotics (particularly those containing methaqualone), are gaining in popularity in Quebec, Ontario and British Columbia. Reports from the Prairies indicate that the non-prescription use of tranquilizers is also increasing in popularity in this region, but that non-barbiturate sedative-hypnotics are generally not available for non-medical consumption.'"
Studies of drug use in Canadian high school populations do not suggest any significant change in the extent of use of sedatives and hypnotics from 1968 to 1971. These studies found that, depending on region, between three and eight per cent of high school students had used barbiturates in the previous six months and that between eight and ten per cent had used tranquilizers during this period of times, 17, 78, 80, 81, 108, 114, 115, 180, 225, 240, 241, 251, 272' 273 While a very recent Addiction Research Foundation of Ontario survey has reported a considerable increase (from 4.3 per cent to 18.2 per cent) in the use of barbiturates among Toronto high school students between 1970 and 1972, the rewording of the barbiturate question in the 1972 survey to include "painkillers" may account for the entire increase. As the authors note: "The results from this question should be treated with caution until further data are available."242
The importance of specifying level-of-use is evident from the data presented in these surveys. A common measure of high frequency use in these studies is more than once a month in the last six months. With considerable uniformity, about one-fifth of those who have used these substances in the last six months have used them once a month or more. This level-of-use could be described as at least occasional, although some unknown proportion of these students may well be heavy regular users. Thus, by 1971, roughly one per cent of high school students in Canada were at least occasional users of barbiturates, and two per cent were at least occasional users of tranquilizers.
A survey of Toronto adults over the age of 17 in the spring of 1971 revealed that nine per cent had used barbiturates in the previous 12 months and 13 per cent had used tranquilizers. This use could be either medical or non-medical use. Thirty-eight per cent of these tranquilizer users and 24 per cent of those who used barbiturates used these drugs every day.82
What proportion of the nine per cent of adults using barbiturates and the 13 per cent of adults using tranquilizers in Toronto use these substances non-medically, at least some of the time? There is no direct measure of this, but there are indirect indicators. We know that about ten per cent of the users, or one per cent of the total population, did not obtain these drugs by prescription. This proportion is similar to the percentage of persons in the Commission-sponsored national adult survey who reported use of tranquilizers without a doctor's supervision: about ten per cent of all tranquilizer users, or two per cent of the total population. However, the Commission survey collected ever used data while the Toronto study was concerned exclusively with use in the previous 12 months. On the basis of these surveys, we may very tentatively suggest that about ten per cent of those Canadians who currently use barbiturates and minor tranquilizers use them without benefit of prescription. This is equivalent to roughly one per cent of the Canadian adult population.
Combining the estimates for high school students (those between 12 and 17) and adults (those 18 and over) yields about 1,380,000 Canadians who have used barbiturates in the past year, and approximately 2,040,000 who have used minor tranquilizers during this same period of time. Of these current adult sedative users, about 180,000 have used tranquilizers and 125,000 barbiturates without a doctor's prescription. Unfortunately, there is insufficient data to estimate the number of Canadian adolescents who have used these drugs non-medically or without a doctor's supervision. However, it is probable that more Canadians use these drugs on a daily medical basis, with a prescription, than use them at all non-medically.
These estimates are based on surveys and, consequently, will under-represent some categories of drug users, for example, heroin or amphetamine users. These persons are known to use barbiturates and minor tranquilizers more frequently than the general population, both non-medically and for self-medication of drug effects. However, their numbers are small compared to those of non-medical users of barbiturates and minor tranquilizers who are available to surveys.
VOLATILE SUBSTANCES: SOLVENTS AND GASES
Volatile substances have always been primarily a pre- and young adolescents' form of intoxicant. These drugs have never been highly regarded in other drug-using circles, and as other drugs (particularly cannabis and alcohol) become available to the 'sniffer', he is likely to shift his preference to them. Glue is no longer the most commonly used solvent. Certain brands of nail polish remover are reported by observers in a number of Canadian cities to be the solvent of choice among these users. Solvent use is now considered an important or increasing drug problem in several parts of Canada, including Nova Scotia and some western provinces. Whether there has been an actual increase in use, or whether this phenomenon has simply become more visible with the increasing attention paid to drug use among young adolescents, is not yet clear.'"
Surveys of solvent use among high school students suggests a stabilization or decline in use between 1968 and 1972. 17, 32, 108, 241, 242, 251, 258, 272, 273 These studies suggest that between five and six per cent of high school students had used solvents in the previous six-month period. Unfortunately, almost all of these surveys are of populations in central Canada. The Commission surveys found that two per cent of high school students had ever used `glue' for psychotropic purposes by the spring of 1970. Other surveys of the
same period suggest that about twice that proportion would have said they had used 'other solvents' if that question had been asked. Of the students in the Commission's high school survey who indicated that they had used glue at some time, three-quarters had not used it in the preceding six months. This suggests a much lower rate of current use of solvents (including glue) than the other surveys, i.e., about 1.5 per cent. Considering the findings of other surveys and the date of those conducted by the Commission, we feel that a safe maximum figure for current use of solvents among adolescents is four per cent. Current use of solvents among adults is considered negligible.
About 20 per cent of these solvent-using students report use of this drug that averages out to more than once a month. In three major eastern Canadian cities, it was found that 62 per cent of student solvent users sniffed `glue' less than three times in the six months preceding the study, while 20 per cent did so seven times or more during the same period.243 A 1972 Toronto survey of high school students found that about one-third of the students who had sniffed 'glue' or other solvents had done so more than one or two times in the six months preceding the study. Less than five per cent of the users reported use of these substances more than 50 times, or an average of at least twice a week, during this same period of time.
TOBACCO
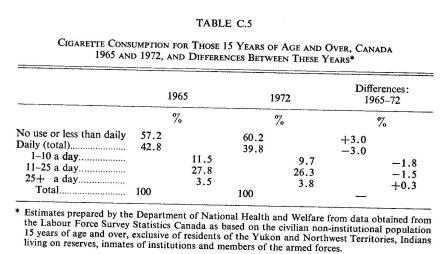
The following table indicates the smoking habits of Canadians 15 years of age and over in 1965 and 1972. During this period there appears to have been a modest decline in the proportion of Canadians smoking cigarettes daily, but the percentage of heavy smokers (those who smoke more than 25 cigarettes a day), if anything, has risen very slightly during these same seven years.
The distribution of cigarette smoking is somewhat atypical as consumption is concentrated at one level-of-use. Almost everyone who smokes cigarettes at all smokes every day, and about 65 per cent of those who smoke at all smoke between 11 and 25 cigarettes a day.
There is little reliable data on the incidence of tobacco use among persons under 15 years of age. However, high school surveys conducted in Montreal and Halifax243 in 1969, in Ottawa108 in 1970, and in Toronto242 in 1968, 1970 and 1972 indicate at least some tobacco use by about 25 per cent of grades seven and eight students and by about 45 per cent of grades nine and ten students. The Ottawa survey, which provides the most complete tobacco use by grade data, shows that 65 per cent of the grades seven and eight smokers consume less than one pack of cigarettes a week, while only about four per cent smoke seven or more packs a week (i.e., at least one pack a day). Among grades nine and ten tobacco-using students, 36 per cent smoke less than one pack a week and about six per cent smoke seven or more packs a week, or at least one pack a day. The Montreal, Halifax and Toronto data do not allow level-of-use analysis by grade or age, but do indicate that between 50 and 60 per cent of the tobacco smokers in these high school populations consume less than one pack, or 20 cigarettes, a week.
Current data regarding the consumption of other tobacco products were not available to the Commission at the time of writing. However, 1964 figures indicate that about 16 per cent of Canadians aged 15 years and over smoked pipe tobacco, and one-half of these persons did so on a daily basis. Similarly, 16 per cent of the 1964 Canadian population smoked cigars, but less than one-fifth did so on a daily basis.