| 59.4% |  | United States |
| 8.7% |  | United Kingdom |
| 5% |  | Canada |
| 4% |  | Australia |
| 3.5% |  | Philippines |
| 2.6% |  | Netherlands |
| 2.4% |  | India |
| 1.6% |  | Germany |
| 1% |  | France |
| 0.7% |  | Poland |
| Today: | 193 |
| Yesterday: | 251 |
| This Week: | 193 |
| Last Week: | 2221 |
| This Month: | 4781 |
| Last Month: | 6796 |
| Total: | 129380 |
| - |
Drug Abuse
CHAPTER XII. EFFECTS—MENTAL.
512. The Commission have attached considerable importance to the inquiry regarding the connection between insanity and hemp drugs because this is the part of the subject of which most has been heard in the past. There has been undoubtedly a popular impression that hemp drugs do cause insanity. There are not a few witnesses who deny this,—who say that they have never seen a consumer of the drugs insane, and do not believe that the drugs ever produce insanity. But the much more common impression is that, at all events if used to excess, the hemp drugs may, and often do, produce insanity. Some few witnesses, generalising from a most limited experience, go so far as to say that insanity is the inevitable result of the use of the drugs. There exists undoubtedly a popular impression which has come down from many generations that there is some connection between hemp drugs and insanity. Besides this popular impression, there has been great prominence given to asylum statistics as affording some tangible ground for judging of the effects of hemp drugs. Over and over again the statistics of Indian asylums have been referred to in official documents or scientific treatises not only in this country, but also in other countries where the use of these drugs has demanded attention. Other alleged effects of the drugs have attracted but little attention compared with their alleged connection with insanity.
513. The popular impression on the subject is capable of very simple explana- tion. I t is undoubtedly a very difficult matter to decide as to the cause of insanity in any case. And it cannot be expected that the popular view of the cause in any particular case should be accepted as accurate. There may be good ground for the popular opinion that insanity is caused by hemp drugs. That question may be deferred for the present. But there can be no doubt that in any particular case this view of causation must be accepted with caution. To ascertain the true cause requires a thorough knowledge of the history of the patient and a scientific capacity for judging of that history. The unscientific or popular mind rushes at conclusions, and naturally seizes on that fact of the case that lies most on the surface. Any exciting cause is more easily apparent to the casual and unscientific observer than a predisposing cause could be. The former is nearer to the effect in point of time, and is naturally more readily associated with it. Similarly, any physical cause is more easily apparent to such an observer than a moral cause would be. The former lies nearer the surface, and any physical fact that seems a possible cause is naturally accepted. Again, an intoxicant would naturally be more readily accepted than other physical causes, because some of its effects as seen in ordinary life are very similar to the symptoms of insanity. This is, perhaps, specially the case with ganja : an excessive dose produces intoxication. Its first effect is the " disequilibration of the intellect," and the mental symptoms of hemp drug intoxica tion are very similar to those of insanity. Such physical symptoms as the casual observer would note are less marked perhaps in the case of ganja than with alcohol, while the mental condition is often that strange mixture of apparent clearness with manifest derangement of thought which is found in insanity, but not usually in alcoholic intoxication. It is only natural that drugs the intoxication of which is seen to produce such symptoms should be readily accepted by the popular mind as a cause of insanity.
This popular idea has been greatly strengthened by the attitude taken up by Asylum Superintendents. They have known nothing of the effects of the drugs at all, though the consumption is so extensive, except that cases of insanity have been brought to them attributed with apparent authority to hemp drugs. They have generalised from this limited and one-sided experience. They have concluded that hemp drugs produce insanity in every case, or in the great majority of the cases, of consumption. They have had no idea that in the vast majority of cases this result does not follow the use. They have accordingly without sufficient inquiry assisted by the statistics they have supplied and by the opinions they have expressed in stereotyping the popular opinion and giving it authority and permanence. All this mass of popular and medical opinion demanded careful examination. The Commission have set themselves to take evidence from lay witnesses and to sift as far as possible the cases mentioned so as to ascertain the basis of the popular view. They have also examined medical men of all classes as to cases of the alleged connection between hemp drugs and insanity which have come before them in their practice, and have cross-examined them carefully in regard to these cases so as to see whether the grounds for the opinion formed in each case are adequate. Finally, they have very carefully considered the asylum statistics, and specially enquired into a large number of asylum cases. It has become apparent in the course of the inquiry that no satisfactory conclusion can be based on the individual cases reported by witnesses. As a rule, it is made manifest at once by cross-examination that the history of the patient has not formed the subject of careful inquiry ; that the opinion is based on most inadequate data ; and that little or no importance has been attached to the question of causation. The Commission have therefore been compelled to fall back on the asylums. This course seems clearly expedient on two grounds—firstly, that the asylum statistics and asylum experience have formed the principal basis of the opinion which calls for examination ; and, secondly, that the asylum cases must form the best material for arriving at a conclusion. In its general effects the evidence of witnesses should not be ignored ; but it is impossible to say precisely what weight ought to be attached to it in regard to particular facts ; and the main basis of any final conclusion must be the material supplied by the asylums which the Commission now go on to consider.
514. The facilities which exist in England for acquiring something like accurate knowledge of the cause of insanity in any par ticular case may be confidently regarded as much greater than those in India. Yet every work on insanity contains comments on the difficulty of arriving at the truth and the unsatisfactory nature of many of the statements recorded. The most important subject of inquiry in this connection is the history of the lunatic's family, so as to discover what (if any) hereditary predisposition to insanity there may exist. Regarding this, Dr. Blandford says (" Insanity and its Treatment ") : " Statistics on this subject are valueless. One author attributes to per cent. of cases to this cause ; another no less than go. This arises from lack of information on the part of some friends and the wilful concealment of others, and also because some statisticians seek for insanity only, taking no account of other neuroses, such as epilepsy or paralysis. If we make the attempt, we shall soon find how difficult it is to get an accurate account of the health of the father or mother and grandfather and grandmother of any one patient." On the wider subject of causation generally, Dr. Hack Tuke (Dictionary of Psychological Medicine ; article "Statistics of Insanity") says : "As the Lunacy Commissioners adopt a classification of the causes of insanity which is fairly workable, and have collected together a large number of returns from English asylums, it is desirable to give the results here for what they are worth. As is well known, the entries made by the friends of patients in the statutory statement are extremely unreliable, and constantly confound cause and effect. The Commissioners state that they have not relied upon these, but upon statements verified by the medical officers of the asylum."
515. If this be the case in England, how much more is it necessary in India to exercise caution in receiving statistics as to the causes of insanity, to examine carefully the source from which they come, and to rely only on those which have been carefully tested. The Commission in examining the statistics of the lunatic asylums soon found that they could not be regarded as trustworthy. They first of all enqiiired into a number of cases in the Dullunda Asylum (Calcutta), and ascertained generally the practice in regard to recording the cause in the asylum registers, and the character of the inquiry on which that record was based. What they learned there led them to distrust the asylum statistics. They determined to make a careful inquiry into all cases attributed to hemp drugs in one year, and to endeavour thus to ascertain how far the statistics were reasonably correct, and, if possible, also to arrive at some conclusion as to whether hemp drugs have any real connection with insanity. They fixed on the year 1892. They considered it for obvious reasons expedient to take the same year all over India ; and this was the last year for which complete statistics existed when they began their inquiry. At the same time these statistics had been completed and printed before the proposal to have any inquiry into the effects of ganja had been made. The Commission decided to take up each of these cases of 1892 separately, and to inquire as fully as possible into its history.
Hitherto any opinion regarding the connection between hemp drugs and insanity which has professed to have any solid basis at all, or to be more than a vague impression, has been based on the figures contained in the annual Statement No. VII appended to the Asylum Reports. It is necessary to consider how far these figures supply any reasonable basis for a scientific opinion on the question.
The figures contained in that statement are compiled from the entries as to cause made in the asylum registers. The great majority of the Superintendents of Asylums have clearly stated that these entries are based on the descriptive rolls sent with the lunatics. They have not considered it necessary to enquire how far the descriptive rolls are likely to give trustworthy information regarding cause, how or by what agency that information is collected, or .by whom it is supplied. It has been sufficient that it is sent to them officially, and that they have no opportunities of testing it. They have therefore accepted it. If the papers have been manifestly incomplete, they have been sent back to the Magistrate for completion. The practically universal rule has beer to accept the cause entered in the descriptive roll, and only to make enquiries in the asylum when no cause had been entered. It cannot be said that even this practice has been carefully and accurately observed. The copying of the entries is left to subordinates who sometimes use their own discretion. Thus Dr. McConaghy, Superintendent of the Poona Asylum, says : "The register is filled up by the assistant at the time of the lunatic's admission. According to my idea of asylum practice, the entries must be in accordance with Form C. If the cause is entered as unknown, it must be so shown in the register. No alteration would be made without the permission of the Magistrate." Yet of the six cases ascribed to hemp drugs in 1892, there was not one in respect to which the entry in the register corresponded with that of the descriptive roll as to cause, and there was nothing on record to explain the discrepancy in any case. Similarly, Dr. Macnamara, Superintendent of the Tezpur Asylum, says : " The cause is entered in the general register from the police statement, i.e., from the descriptive roll. We have nothing whatever to do with it. It is entered by the Overseer in charge of the Asylum, and ought to correspond with the entry of the descriptive roll." As a matter of fact, eleven of the thirteen cases for 1892 showed entries regarding cause which did not correspond with the descriptive rolls; and of these 11, no less than lc) were made, not by the Overseer, but by his subordinate, the jemadar. Besides such errors as these, there are errors arising from carelessness in the mere copying of the register entries from year to year. These derive their importance from the fact that they must have been discovered had any attention been really given in the asylums to this matter of causation. A striking example may be given from 'among the old cases in the Rangoon Asylum. Moung Min Thay was admitted on 25th June 1871. There has been no improvement in his mental state. There are no papers in his case except an order from the Magistrate to receive the man " supposed to be in. sane." The original entry in the case book shows cause as " predisposing disease of the brain, exciting drinks, and smokes opium ;" and it shows the duration af. " probably from birth." It also shows that the man was epileptic. There is no mention of ganja. The register for 1885 (the first to show causation) shows " alleged duration " as " congenital," and " alleged cause " as " drink and opium smoking." The entry " congenital " is continued until 1892, when it is replaced by a "Do." under the " Not given " of a previous case. In 1886 the " cause " similarly undergoes undesigned alteration. The word " drink " is replaced by " ganja ;" and in 1888 the reference to " opium " is finally dropped. The case thus became a ganja case, and has been shown as such ever since. These all may be instances of exceptional carelessness, but as a general rule it cannot be said that these entries have been made with care. Superintendents have not attached much importance to them. It has been left to subordinates to do this work ; and that work as a rule has not been carefully supervised. Speaking generally, however, Superintendents have desired that the entries in the register regarding cause should correspond with those in the descriptive rolls ; and they have believed that their subordinates were making the entries on this principle.
Some few Superintendents have professed a different method, and have assumed some responsibility for the entries as to the cause of insanity in their registers. There are, however, only three Superintendents who held this office in 1892 who profess to have been to any appreciable extent independent of the police statements or descriptive rolls. The first of these is Brigade-SurgeonLieutenant-Colonel Hooper, who says that his "practice has not been to enter the cause at once, but to wait until a diagnosis of the case has been made. Then, if the supposed cause, as shown in the Magistrate's statement, is not inconsistent with the diagnosis of the insanity, or with the information received from friends who may have come, or with statements made by the man himself if he recovers sufficiently, that cause is entered in the register." The part played by diagnosis in the determination of cause is, however, somewhat visionary ; for Dr. Hooper says that there are no symptoms peculiar to hemp drug insanity except perhaps more speedy recovery, and that an accurate history is " absolutely essential ; it is the only means by which you can arrive at a diagnosis." As to the statements of friends, Dr. Hooper seems to think that friends visit patients in the majority of cases. If this is so in Lucknow, his experience differs from that of Superintendents elsewhere. It is possible, however, that he may be mistaken, for it appears that enquiries from friends are " not ordinarily " made by him, but by the Deputy Superintendent. The statements of lunatics also appear from his evidence rarely to affect the entries. There is one point on which Dr. Hooper specially insists, viz., that any fact established regarding heredity would exclude the ganja theory. Turning to the cases for 1892, it is found that there was one case in which the lunatic's brother was insane, and another where a direct ancestor was insane ; but no notice was taken of these facts in determining cause, and the cases were entered as due to hemp drugs. It also appears that in 14 out of the 17 cases shown as due to hemp drugs, this cause is entered in accordance either with the entry in the papers regarding cause, or with that regarding the lunatic's habits. Of the remaining three cases, there is in one an alleged statement by the lunatic's brother (afterwards denied). In another the lunatic "recognizes bhang and makes contradictory statements as to its use." In the third, there is the statement of the lunatic himself while still insane.
The second Superintendent who states that he adopts exceptional practice is Brigade-Surgeon-Lieutenant-Colonel Keith of Hyderabad (Sind), who says that " the only ground, so far as I can remember, on which I would enter cause would be information of friends or the statement of the insane after he had recovered his wits." It is striking that of the 13 cases set down to hemp drugs in 1892, the cause as entered in the register corresponds in 1 o cases with that entered in the papers sent with the lunatic. In the other three cases no basis for the entry of cause is given at all. In one case the Superintendent told the members of the Commission who visited the asylum that the entry was based on a statement made by the father ; this the father now denies. In the other two cases, no such explanation was given by Dr. Keith to the members of the Commission ; but that officer now says (probably on the authority of some subordinate) that these two lunatics used to ask for the drug in the asylum. No record of any such fact was found in the register. The Commission are unable in view of all that has been ascertained of these cases to attach much weight to these statements.
The third exceptional case is that of Surgeon-Major Dobie of Madras. In his letter of loth October 1893 (vide Vol. II Appendices) Dr. Dobie said : " I am responsible for the entry of the cause as ganja in the first 14 cases [of 1892]. In no case have I entered it as a cause without such evidence as led me to a reasonable belief that it was so." But in his evidence before the Commission on 22nd January 1894, this officer stated : " My reasonable belief as to cause was based on reading the papers and seeing whether they showed a probable cause of insanity, and on enquiry from the lunatic....... I feel very little confidence in the diagnosis I have made ascribing these cases to hemp drugs."
516. There is clearly no valid ground in the practice of these three Superintendents for modifying the general statement based on the frank admission of the great majority of the Superintendents that the entries regarding cause in the registers, and therefore the figures in annual Statement .No. VII, have been based wholly on the descriptive rolls or similar papers received with the lunatics. This practice has, no doubt, become established owing to the following considerations. As already stated, many Superintendents have recognized these papers as practically the only material they had for determining cause. They have not had adequate opportunities for making enquiries themselves. They have had a general impression that the information supplied by Magistrates or police was as good as the Government required for statistical purposes, and they have accepted it accordingly. Asa rule they have regarded this question of cause as one of little or no practical importance. The Government prescribed Statement VII, and pressed to have the columns filled up ; and as a rule the orders were carried out in this somewhat mechanical way. Surgeon-Major Carruthers, Superintendent at Calicut, perhaps puts this view in the strongest terms when he says : " My position as Superintendent of the Lunatic Asylum requires me to take charge of insanes when they are sent in, and retain them until they are fit for discharge. I am simply keeper and incidentally medical attendant, and not responsible for any statements and certificates received with the patient so long as they are in order. " The same view is, however, as clearly expressed by Brigade-SurgeonLieutenant-Colonel Hooper when he says : " I do not consider that the question of cause is one which affects the treatment of cases. My inquiries therefore into cause are of a statistical, not a practical, character. The result will not affect my treatment of the case." Even to an officer who sees that the knowledge of the cause may help him in the treatment of the case, responsibility for the accuracy of the returns is a very minor matter. Surgeon-LieutenantColonel Leapingwell (Vizagapatam), for example, says : " The point, of course, is chiefly one of personal interest to me in the treatment of the case. An entry was made (in the particular case under discussion) on the papers. I omitted to alter the register." It is clear then that the medical officers in charge of asylums have not felt that they have been in any way responsible for the accuracy of the figures contained in annual Statement VII regarding causation of insanity ; and that these figures derive no value from the fact that the statement bears the signature of a medical man ; for their value practically depends entirely on the character of the inquiry in which the information contained in the descriptive roll was in each case collected.
517. This inquiry is very unequal in its character. The lunatic, before being sent to the asylum, is for a time under the observation of the Civil Surgeon. The latter has to certify to the man's insanity and to the facts which have led to that conclusion. Sometimes the Civil Surgeon fills up the descriptive roll as well as the medical certificate. But the more general practice is that he confines his attention to the medical certificate, leaving the descriptive roll, which contains all that is known of the lunatic's history, to be filled up by the Magistrate or the police. Where it is the practice for the Civil Surgeon to fill up the descriptive roll, the entry regarding cause is made by him or under his orders. Even in that case, however, he is generally compelled to accept the statements of the police. The majority of the lunatics sent up are wanderers who have no friends. Friends, even when there are any, are averse to appear lest they should be called on to contribute to the support of the lunatic. The following statements may be taken as typical of the usual experience of Civil Surgeons in this respect : " As Civil Surgeon, I got the information from friends or from the police. Very often I had cases where no friends came. In such cases I trusted to the police or wherever I could get my information " (Surgeon-Major Boyd, Colaba). "The information I give in Form C is generally very incomplete, as I have only the lunatic to get it from " (Surgeon-Major Burke, Poona). " The friends very rarely attend. As a rule, then, I am left entirely to the statement or form received and to the police" (Surgeon-Major Emerson, Bareilly). Thus, even where the Civil Surgeon signs the descriptive roll, he bases his entries therein as a rule on information supplied by the police. The more general practice is therefore also the more correct, to have the descriptive roll formally filled in by the police and signed by a Police officer or Magistrate, as the police supply the information. The inquiry into the history of the case is not an inquiry conducted by a professional man from the persons likely to know most about the lunatic. The information consists often merely of the guesses of police officers as to the history and habits of a friendless and homeless wanderer ; and in other cases, where a local inquiry is possible, it is generally made by a subordinate police officer.
" I am aware," says the Surgeon-General of the Bombay Presidency, " that inquiries in these cases are generally conducted by a subordinate officer of police." Surgeon-Captain Walsh, of the Calcutta Asylum, says : " The descriptive rolls are filled up as a rule by a Native Police Inspector on the information of a native policeman." Surgeon-Lieutenant-Colonel Bovill, of Patna, goes further. He says : " The statements in the descriptive rolls regarding cause are as a rule not very reliable. I cannot say what grade of police records them. But I think the information is often in small villages brought by chaukidars." Surgeon-Lieutenant-Colonel Crombie, Superintendent, General Hospital, Calcutta, says : " The inquiry is made by the police. I have myself seen an inquiry going on in which a constable was filling in the papers from the statements of the lunatic himself, the man being at the time insane. This may be exceptional, but I have seen it. In any case I distrust this descriptive roll." These are some typical statements regarding the agency which, as a rule, collects the information on which the asylum statistics as to cause are based. Sometimes, as at head-quarters, the inquiring police officer may be an Inspector ; but, as a rule, he is very subordinate. It is impossible to share the cheerful optimism of Surgeon-Lieutenant-Colonel O'Brien, of Benares, who says that "when ganja is assigned, the man was probably 2 notorious ganja smoker. The inquiry may be conducted by a chaprassi, yet he might be right in that." It would be absurd to accept without great distrust the statements, especially as to the cause of insanity, compiled by such an agency as has been described. This distrust of the descriptive roll is intensified when the source of the information is considered. If the police think it worth while, or find it possible and convenient, to make anything of the nature of an inquiry, they find that they have to be satisfied with the very poorest material. Sometimes, as shown. above, it is the statement of the lunatic himself while still insane that is recorded, not only as to history and habits, but also even as to the cause of his insanity. Often, as in the case of garden coolies in Assam or wandering mendicants all over India, it is the statements of mere casual acquaintances who know little of the lunatic's habits and nothing of his past history or of that of his family. Even when friends are found from whom inquiry can be made, they are generally of the most ignorant and unintelligent type. It is from the classes of such a type that most of the inmates of our asylums are taken. It is very rare indeed to find one of the higher and more intelligent classes. The ignorant and uneducated persons who ascribe a child's epilepsy to his having accidently touched the painted stone that represents the village god while playing under the sacred tree, or a fit of insanity to the attack and possession of a blnit or village ghost, who know nothing of causality, except in the most ordinary affairs of home or agricultural life, beyond the mere association of coincidence, who believe in no cause which they do not see except witchcraft, whose powers of observation are quite unexercised and undeveloped : such persons must form most unpromising material even for the most patient and intelligent enquirers to work on. The information gleaned from them by such agency as has been above described must be of the most incomplete and unsatisfactory character. It is not surprising that moral causes of insanity, being much less palpable than physical causes, should sometimes be overlooked. A much more surprising fact is the ignoring of many physical causes. Dr. Wise, then Superintendent of the Dacca Asylum, gave a remarkable illustration of this in his report for 1872 : " It is a curious circumstance that in Bengal insanity is never traced to blows on the head, which in Europe is a not infrequent cause. This is the more surprising, as there are few races, I believe, who so commonly have marks of blows on their heads as Bengalis. Out of 190 males in the asylum on 1st January last, 57 (or 30 per cent.) had more or less extensive scars or cuts or contusions on the head. In a considerable proportion the blow must have been so severe as to have caused violent concussion of the brain. Yet in the records of this asylum there is no instance of insanity attributed to this cause."
Finally, the distrust of the descriptive roll must be further intensified by the consideration of the pressure brought to bear on subordinates to supply Information as to cause. An illustration of this may be found as early as 1863 in the Resolution of the Government of Bengal on the Asylum Reports for 1862. And a striking illustration of the effect of this pressure is found in the Dullunda Asylum returns for the following year (1863), in which the cause in several cases dating from the year 1857 and onwards was altered from " unknown" to "ganja smoking." The same pressure is still brought to bear on those responsible for the entries of cause. Surgeon-Major-General Turnbull, the head of the Medical Department in Bombay, says : "There is a column in Statement VII headed " Unknown" which is intended for the entry of cases in which the cause has not been ascertained with reasonable accuracy. If this column was largely used, I shOuld think it would be a matter of censure on the person on whom the responsibility for inquiry rests." This demand for much information where little information is available, and this insistence on ascribing a cause where reasonable presumption as to cause is so rarely possible, have had a powerful influence in rendering the statistics untrustworthy. The same tendency is seen at work in other provinces. In Madras the effect of the remark in paragraph 5 of the Government Resolution on the Lunatic Asylum Report for 1890 stigmatizing the Calicut Asylum as " the worst " in respect to the average of unknown causes and of the Surgeon-General's Circular No. 12, dated 28th September 1891 (issued in consequence), is clearly in evidence. In Bengal, Surgeon-LieutenantColonel Meadows, of Berhampur, says : "We assign cause too often ourselves : it is insisted on ; and we are constrained to enter cause before it has been properly ascertained." Surgeon-Major Baker, of Rangoon, says : " I think that officers are under the impression that it looks as if they were not zealous if they do not find a cause." Brigade-Surgeon-Lieutenant-Colonel Gaffney, of Jubbulpore, says : " I think that there is a tendency, to assign causes too readily ; " and he intimates his concurrence in a strong protest made by Surgeon-Major-General Rice when Civil Surgeon of Jubbulpore in 188o against this tendency. In Assam, Mr. Driberg, Commissioner of Excise, says : " If a man (policeman) does not enter cause, I know by experience that the District Superintendent of Police gets a slip telling him to send a more experienced man, or fine this man for carelessness." The remarks made in 188o by Dr. Rice, now Surgeon-General with the Government of India, in reference to an unfavourable comment in the Chief Commissioner's review of the report for 1879, may be quoted : " I think it is of doubtful value," he said, " to set down everything told in this way as if it were reasonably true. If these returns are ever to be made use of, it would be better to assign only such alleged causes as have some pretensions to being correct, omitting altogether those which are nothing more than mere conjectures. Even if a great number go unclassified, it is better so than that doubtful causes should be assigned."
518. There is one class of cases which seems at first sight to differ from the rest, the cases in which lunatics charged with crime have been acquitted on the ground of insanity..
Surgeon-Major McKay, of Nagpur, says : " In criminal cases the cause is generally taken from the judgment of the Court." This statement is apparently too strong. The Commission have had to examine the records and papers in the cases of many criminal lunatics. In the majority of cases the Judge is found to be content with the evidence of the Civil Surgeon as to the fact of insanity, and to consider it unnecessary to make any inquiry as to cause. In such cases the information sent to the asylum authorities is precisely of the same character as that furnished in non-criminal cases. It is very rare indeed that any evidence as to cause appears in the evidence tendered in Court, and still more rare for the Judge to discuss the cause. For all practical purposes, the remarks above made regarding the untrustworthy character of the information supplied to the Superintendents, and of the asylum statistics as to cause based thereon, apply to all classes of cases.
519. Although these statistics have been discussed seriously from year to year, they have not been much used as the basis of measures of ganja administration except in the case of Burma. In this case the Commission found that the measures taken
in Burma were ostensibly based on the lunatic asylum returns which were quoted by more than one Chief Commissioner, special reference being made to the figures for the Dacca Asylum. This special reference to this asylum and the fact that it is situated in the most important ganja-consuming tract in India were among the reasons why the Commission summoned Surgeon-Lieutenant-Colonel Crombie (Bengal witness No. 104) as a witness; for he had been seven years Superintendent of that asylum. Before the Opium Commission also, and in an interesting discussion on opium published as a Supplement to the Indian Medical Gazette of July 1892, Dr. Crombie had incidentally spoken strongly of the evil effects of hemp drugs as seen in his asylum experience. The Commission hoped therefore that Dr. Crombie might be found to have devoted special attention to his asylum work, and to be able to speak with exceptional authority. He informed the Commission in his written evidence that " nearly thirty per cent. of the inmates of lunatic asylums in Bengal are persons who have been ganja smokers, and in a very large proportion of these I believe ganja to be the actual and immediate cause of their insanity. But though I am not prepared to say that the moderate use of ganja is never the cause of insanity, it is most frequently the result of long excessive use, and especially of occasional debauches with the drug. It has the same relationship to insanity in India that alcohol has in Europe, and may be the cause of fierce maniacal excitement of short duration (as in delirium tremens) or of a chronic cheerful mania which is the characteristic insanity of Indian asylums. It has not the same tendency to lead to dementia, the result of tissue changes in the brain, as alcohol has. Like alcohol, it will especially lead to insanity in persons of deficient self-control who take to the drug as a relief from mental trouble. Both forms of ganja insanity, the acute and chronic, are distinguishable by the symptoms. (See separate memorandum.) "
These views, which are stated in greater detail in a separate memorandum, are based entirely on his experience as Superintendent of the Dacca Asylum and as visitor to other asylums ; for Dr. Crombie says: " In my practice outside of lunatic asylums my experience is confined to very few cases, only two or three in the whole course of my service, of ganja intoxication brought to hospital." The Commission were anxious to ascertain how far these views might be regarded as having authority. They accordingly examined the registers and case books of the Dacca Asylum for all the years during which Dr. Crombie had been Superintendent, and perused his reports. They were unable to find in these records any ground for thinking that Dr. Crombie's practice differed from that of other Asylum Superintendents, or gave him special opportunities of knowledge. They took the registers for these years and also the papers for all the hemp drug cases of 1887 (Dr. Crombie's last year at Dacca) to Calcutta to discuss them with Dr. Crombie. That discussion is contained in the record of his oral evidence.
First, as to procedure, Dr. Crombie told the Commission that the descriptive roll is " by no means trustworthy," but that " subsequent discoveries" were made in the asylum by examination of friends or of the lunatic on recovery and by other means, and that the entries in the asylum books would be altered accordingly. " This," he said, " was my practice." The Commission had found no trace of this practice in the asylum records ; and they showed Dr. Crombie the registers and asked him to point out any such alterations. He then withdrew his statement, and accepted as accurate the statement of Rames Chandra Sib, Overseer of the Dacca Asylum, who has made the entries in the registers and compiled Statement No. VII ever since 1880. His statement is ; " The cause is entered in the register from the descriptive roll Cause is never entered in the register from enquiry made after the patient's admission. I know of no case of this being done. The entry made at the top of the page would never be altered. But if any enquiry which I might make showed cause not hitherto known, this fact would be entered in the history of the case. I remember such cases, and I might be able to point them out. But that entry in the history of the case would not alter the cause as shown in Statement VII of the annual report. That statement is filled up only from the entries made in the descriptive roll as copied into our register." Dr. Crombie's procedure then differed in no respect from the most mechanical and unintelligent record of causation in any asylum in India, for it was left entirely as clerical work to a subordinate. And the only statistics on which Dr. Crombie bases his views regarding insanity rest on the descriptive rolls, of which he strongly declares his distrust.
Secondly, in regard to Dr. Crombie's attention to the special matter of causation of insanity, it appears that " there was no discussion of cause in any annual report written by him from Dacca, nor any formal discussion in writing." Like other Superintendents, he seems not to have felt that his duty required special attention to this subject.
Thirdly, the Commission discussed with Dr. Crombie the cases of 1887, and the results of this discussion of them are recorded in his oral examination. They afford clear proof of the fact that even a careful examination of the papers received with the lunatics on their admission would have prevented five out of the fourteen cases being recorded as hemp drug cases (viz., the first, fourth, tenth, thirteenth, and probably also the twelfth), and would have led to two • more being recorded as mixed or doubtful cases (viz., the second and fourteenth). The history in the asylum should have prevented the fifth case being retained as a ganja case; for the true cause (peripheral irritation) was clearly established, and insanity was cured on removal of that cause. It should also have led to the rejection of the eighth case, or at least to its being recorded as a mixed case. Thus nine out of the fourteen hemp drug cases of 1887 at Dacca are found to have been erroneously entered as such. There remain only five true hemp drug cases. Dr. Crombie says : " Taking my whole asylum experience, I think that this may probably be accepted as fairly representative of the real state of the case." The total admissions in 1887 to the Dacca Asylum were 55. Of these Dr. Crombie now accepts only 5 (or 9 per cent.) as due to hemp drugs. And he states that this may be accepted as fairly representative of the real state of the case, so far as his experience enables him to judge.
Fourthly, as to Dr. Crombie's conclusions. As there were fifty-five admissions into the asylum in 1887, the number of cases (five) which may reasonably be attributed to ganja turns out to be only nine per cent. As Dr. Crombie says that the " chronic cheerful mania" which he describes is only found in a portion (or, as his separate memorandum shows, in a minority) of the admissions, and as he admits that it " may be due in part to difference of character " and not to the drug, there does not seem to be,much, if any, ground for associating this chairomania with hemp. And in view of the small proportion of true hemp drug cases and the large proportion (nearly 2 to t) of error in the cases accepted and recorded as hemp drug cases in Dr. Crombie's time too much weight should not be attached to his views regarding the clinical features of hemp drug insanity. The results of a careful analysis and examination of his cases corresponds on the whole pretty accurately with the examination of the cases of 1892 for all India made by the Commission. Looking back at his work in Dacca from his present point of view, Dr. Crombie seems:to have thought that he had had some experience of special value, but the impression appears on examination to be due to a mistake of memory. There is practically nothing that differentiates his experience or the practice of the Dacca Asylum from that of other Superintendents and other asylums in India.
520. It may well seem extraordinary that statistics based on such absolutely untrustworthy material should have been submitted year after year in the asylum reports. It is extraordinary, and cannot certainly be fully justified. The following considerations serve to a certain extent to explain this extraordinary fact. In the first place, as is pointed out by several Superintendents, these officers did not know what grade of police or what kind of agency was employed in the inquiry. They believed that they were bound to accept, and justified in accepting, without question what came to them with an appearance of official authority. In the second place, all the Superintendents, except those in the towns of Madras and Bombay, have their asylum work in addition to other medical duties. They have found themselves unable to devote that amount of time and care to their asylum work which would enable them to speak as experts or to supply information of any real value. Some of the best of them have stated to the members of the Commission who visited the asylums that they constantly found themselves subordinating the asylum work to duties which appeared more pressing and more important. In the third place, as already pointed out, they have been so pressed to give statistical information that they have often done so without considering whether it could be regarded as scientifically or even reasonably accurate. In the fourth place, most of the Superintendents, though they had long practised medicine in this country, had never seen any of the effects of hemp drugs except their alleged effects in producing insanity in the cases attributed in the papers to the drugs. Several Superintendents speak clearly of this ignorance of the effects of the drugs. The remarks of three may be quoted as being specially interesting. Surgeon-Lieutenant-Colonel Leapingwell (Vizagapatam) says : " I should myself have put down ganja as the cause of insanity in any case where I examined the friends if they merely said the man used ganja and I could get no other cause, as I did not discriminate between the excessive and moderate use. I should go much more carefully into the matter now, since I have in the course of the present inquiry learned so much more about the use of the drugs." Surgeon-Major Cobb, of Dacca, says : " As to the effects of ganja generally, I should say that until I began to study the question with a view to give evidence before the Commission, although I had a vague notion that ganja smoking was prevalent among the lower classes in Bengal, I had no idea that the practice was as common as I have since found it to be." Surgeon-Major Willcocks, of Agra, says : " Ordinarily it has been the practice to enter hemp drugs as the cause of insanity where it has been shown that the patient used these drugs. I cannot say precisely why this is the practice. It has come down as the traditional practice. As a matter of fact, until recently I looked on these drugs as very poisonous. As I have already said, my ordinary medical practice did not bring me into contact with them at all. I only came into contact with them in the asylum. I had no idea that they were used so extensively as I find on enquiry to be the case. I have made enquiry in connection with the attention drawn to the matter recently."
These are some of the explanations which may be offered for the submission by Superintendents of such statistics year by year. Further, though such evidence as that of Surgeon-Major-General DeFabeck of Madras shows most clearly how little knowledge some heads of the Medical Department have had of the untrustworthy character of the statistics, it does not show this more clearly than does the mere fact that year after year these statistics have been seriously discussed alike by these officers and by the Governments under whom they serve.
521. The Commission were forced to the conclusion that there was no trustworthy basis for a satisfactory and reasonably accurate opinion on the connection between hemp drugs and insanity in the asylum statistics appended to the annual reports. They felt that they must conduct for themselves as full and searching an inquiry as was possible within the time at their disposal into the history of a considerable number of cases. As already stated, they selected as the subject of their inquiry all the cases admitted into all the asylums in India in 1892 and ascribed to hemp diugs. They took up each of these cases separately in the asylum, and ascertained what information was obtainable in regard to it from perusal of the original papers and the asylum registers, and also by enquiry from the Superintendent and Asylum officials. Having recorded all such information, they asked the Superintendent of each asylum to conduct further inquiry into each case and report finally on it, and they requested Local Governments to direct the Magistrates and Civil Surgeons of districts to which the patients belong to give the Superintendent all necessary assistance. The CoMmission added : " In view of the importance of this branch of the inquiry, it is suggested that, wherever this is possible, a careful local inquiry should be conducted by a trustworthy and experienced Magistrate, in consultation with the Civil Surgeon, to ascertain the past personal and family history of the patient, and any circumstances likely to throw light on the cause of his insanity. The record of this inquiry should in each case be submitted to the Commission through the Superintendent of the asylum in which the patient was treated to enable him to submit the report above mentioned. " All this information, both that collected in the asylums and that collected in these further inquiries, is recorded in Vol. II Appendices. Only the final report of the Superintendent is printed, unless it is inaccurate or incomplete, or unless there is anything of interest in the records which he has not noticed. In these cases notes containing the points omitted or inaccurately stated, or extracts from the records, are appended to his report. Prefixed to these papers is a statement of the decision of the Commission on all of the cases, showing very briefly for each why it has been accepted or rejected. In a few cases the results of the inquiries are unsatisfactory ; for it has been impossible occasionally to get any further information ; and occasionally the inquiry, even though feasible, has not been conducted with sufficient care and intelligence. On the whole, however, the result is the collection of a body of information about these selected cases far superior to anything heretofore available.
The result of the examination of all the cases attributed to hemp drugs in 1892 may be thus shown :—
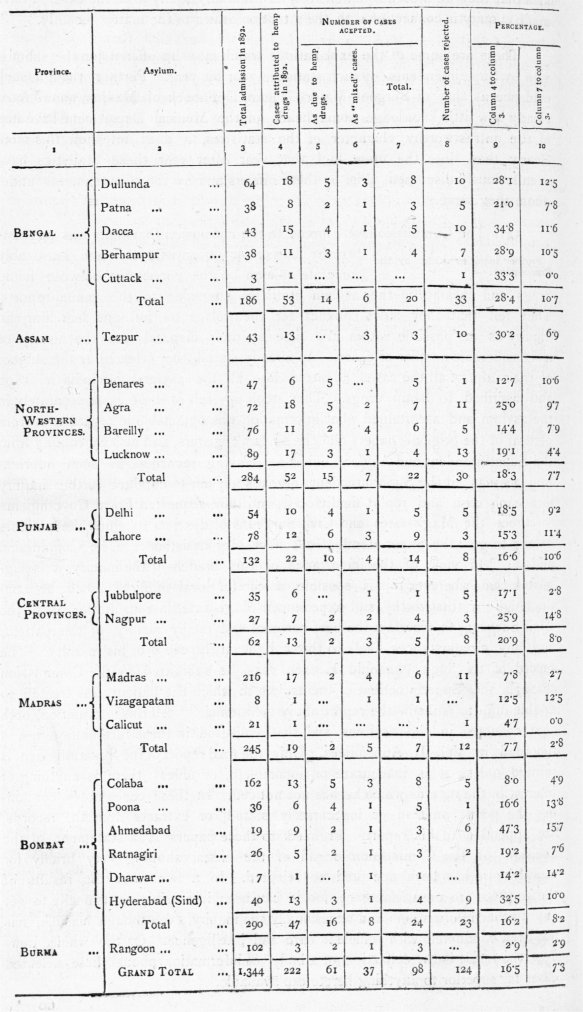
Out of 1,344 admissions to the asylums of British India during 1892, there are shown to be only 98 cases (or 7'3 per cent.) in which the use of hemp drugs may be reasonably regarded as a factor in causing the insanity. If the " mixed " cases in which the hemp drugs have only been accepted as one of several possible causes are omitted, the percentage falls to 4.5. It must be borne in mind, however, that there were 42 per cent. of the admissions for 1892 in which the cause of insanity was shown as " unknown." Among these " unknown " cases there may, no doubt, have been some in which hemp drugs may, as in the accepted cases, have played some part in causing insanity. If it had been possible to ascertain the history of these " unknown " cases, it might have been found that there was in a considerable number of them a history of the use of hemp drugs, and perhaps that in some of them these drugs had played some part at least in causing the insanity. It might appear at first sight to be more correct to take the percentage, not on the total admissions into the asylums, but on the " known" cases among these admissions. The total number of " known " cases (i. e., cases in which the cause was supposed to be known) among the admissions for 1892 was 775. This would give a percentage of hemp drug cases at 12.6. But the Commission do not see their way to accept this method of calculation as accurate. For they consider that both experience and the whole history of this inquiry have shown that there is little difficulty in ascertaining the existence of the ganja habit among persons such as are sent to the asylums, and also that there is no hesitation in ascribing insanity to that habit. They are therefore of opinion that it is safe to presume that in the great majority of the " unknown " cases no ganja habit did exist, and that they would be further from the truth in taking the percentage at 12.6 than at 7.3.
522. On the other hand, it would be far from accurate to say that it has been ascertained that the insanity was in all these 98 cases due solely to hemp drugs. In the first place, there are 37 of them (or nearly 38 per cent.) in which there is a clear history of some other cause. The causes which are shown thus to have possibly co-operated with hemp drugs in inducing insanity (with the number of causes for each) are as follow :-
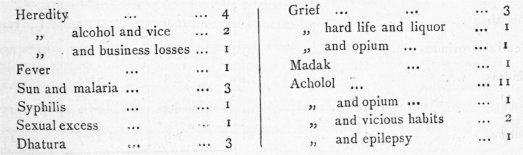
523. Only a few remarks need be made regarding these " mixed " cases. So far as the inquiries have established the real facts regarding these cases, there are seven into which heredity enters as a predisposing fa ctor. The number of cases attributed to heredity throughout India in 1892 was 51, or 3'8 per cent. of the admissions (1,344). These seven cases may perhaps be added to this number, giving a total of 58, or 4.3 per cent. In England the percentage of cases attributed to heredity is 19'o for males and 22'1 for females. These percentages are based on statistics for ten years, dealing with 136,478 patients (vide Hack Tuke's Dictionary of Psychological Medicine ; article " Statistics of Insanity "). The adthor of this article points out that " the reluctance of the relatives of patients to give information on this painful point leaves the proportion undoubtedly far too low." In view of this, it cannot be denied that the influence of heredity is in India practically neglected. The importance of giving due weight to this factor becomes the more manifest when it is considered that a cause which in a normally healthy brain would produce no effect is sufficient to overthrow the mental equilibrium of a person with hereditary predisposition.
524. There are eighteen of these mixed cases in which alcohol has been ascertained to be a possible factor. In view of the connection between alcohol and insanity as established in Europe, and in view of the clear evidence that brain lesions are directly caused by alcohol, there seems certainly not less reason for ascribing these cases to alcohol than to hemp drugs. The English statistics show percentages of 19.8 and 7'2 of cases as due to alcohol for males and females respectively. The Commission are of opinion that such high percentages cannot be expected in India ; for, although the action of alcohol is more injurious in the tropics, the people of this country are generally much more abstemious. The percentage of cases attributed to alcohol in each province in 1892 is given below, and for purposes of comparison the percentage of the accepted hemp drug cases (including the " mixed " cases) is also shown :—
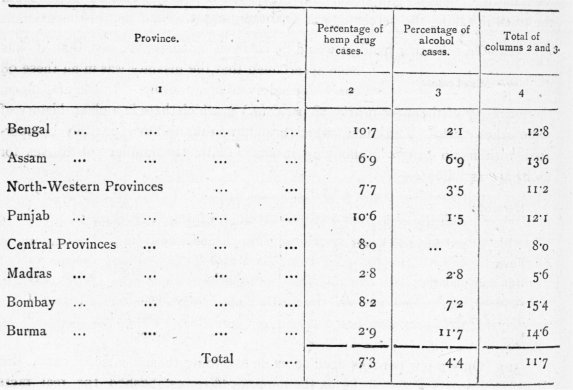
The figures in regard to alcohol cannot be accepted as quite satisfactory, because they have not been tested. But the tendency of the figures as they stand is to show that in the provinces where hemp drugs are the less used, alcohol is the more frequently assigned as the cause of insanity, and vice versd. It is possible either that the figures to a certain extent reflect the facts, or merely that those who have to account for insanity turn most easily to intoxicants, and came that intoxicant which most readily occurs to them.
525. There are three " mixed " cases in which dhatura has been ascertained to be a possible cause of insanity. In view of the facts that dhatura is a more potent intoxicant than the hemp drugs and produces furious delirium, and that Dr. Cunningham's experiments appear to indicate clearly that grave cerebral lesions are very early produced by dhatura and are not produced by ganja, it would probably be safer to accept these cases as due to dhatura and not to hemp drugs. The Commission have, however, accepted them as " mixed " cases. It is unnecessary to make any special remarks on the " mixed " cases in which causes other than heredity, alcohol, and dhatura appear to contribute to the insanity.
526. Even in regard to the remaining 61 cases, it must be borne in mind that it is impossible to say that the use of hemp drugs was in all the sole cause of insanity, or indeed any part of the cause. The following considerations combine to demand caution and reserve in pronouncing an opinion on this point.
Firstly, there are twelve cases in which it has been found impossible to obtain any further information by local inquiry. In these cases we are thrown back on the original papers and the asylum history. Besides these, there are ten more cases in which the patients are beggars and foreign labourers about whose past history no satisfactory information is obtainable. Thus there remain only 39 of these 6i cases about which anything like a satisfactory inquiry has been possible. Further, a great majority of these cases come from the lower orders of cultivators and labourers, from whom information of any value is very difficult to obtain as to other than the most apparent causes. The fact of the existence of the hemp habit is easy enough to ascertain, but that it is the cause, or one of the causes of the insanity, or that it even preceded the insanity, is much more difficult to establish.
Secondly, the method of inquiry has not been satisfactory in regard to all the cases referred for local inquiry. In regard to the great majority, the instructions issued by the Commission as to the agency by which this further inquiry should be conducted have been carried out. But in some, it will be observed, even this further inquiry has been left to the police. Then again there are cases, such as those of the Hyderabad (Sind) Asylum, in which the Superintendent has necessarily been the principal agent in the inquiry, and has, perhaps, not unnaturally, but certainly unfortunately, evinced a strong tendency to defend the old asylum entries regarding cause. The series of questions framed by the Civil Surgeon of Delhi for use in the further inquiry also illustrates a tendency to assume that the cases were hemp drug cases, and thus to limit the scope of the inquiry.
Thirdly, it may be noted that excess in the use of hemp drugs is very frequently only one of several vices in which a dissipated man indulges. Further inquiry has proved this in several cases. There is strong probability that had information been complete, it would have been established in many more cases. It is impossible in such cases to say definitely to what form of excess insanity may be mainly clue. Further, it is an accepted and established fact that intemperance of any kind may sometimes be not the cause of insanity, but an early manifestation of mental instability. Dr. Conolly Norman (Hack Tuke's Dictionary of Psychological Medicine ; article " Mania ") says : " The patient also indulges in intoxicants with very undue or unwonted freedom, and thereby precipitates the course and aggravates the symptoms of his disease." One or two cases have been rejected by the Commission on the ground that the evidence merely showed that the habit of use of hemp began at the same time as the mental aberration, or even later. There may have been other cases in which this would have been shown had the information been complete. It is possible therefore that more complete information might have shown in some cases, not only that other causes contributed to the insanity, but also that hemp drugs had nothing whatever to do with inducing it.
These and similar considerations already indicated demand caution in the expression of any judgment as to the causation of insanity in this country. If in England opinion, based on inquiries such as are there possible, has to be stated with caution, this is much more necessary here. In many of the cases in which the hemp drug habit has been established, it is impossible to feel certain in view of the defective character of the information that the drugs have been the sole cause, or perhaps indeed a cause at all, of the insanity. The Commission have, however, felt themselves justified in accepting these 98 cases of the year 1892 as reasonably attributable, in whole or in part, to the use of hemp drugs. These are the best cases they have been able within the time at their disposal to obtain. Of these 98 cases, 97 were males and one female, 82 being Hindus and 16 Muhammadans.
527. In the asylum returns these cases were classified according to the following " types " :—Toxic insanity, 39; mania, 42 ;melancholia, 3 ; dementia, 4 ; while in ten cases the patients had recovered prior to admission, and did not exhibit symptoms of mental aberration while in the asylum. The Commission think it well to point out that although in these instances symptoms of insanity were never observed by the Asylum Superintendents, yet the cases were returned in the annual reports as-cases of toxic insanity, and thus helped to augment the annual returns (Statement VI)--a fact which very strikingly exemplifies the purely mechanical manner in which these returns have hitherto been compiled.
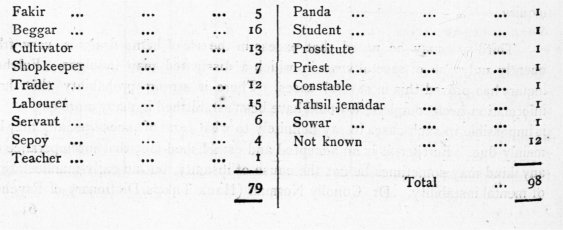
528. The occupations, etc., of these 98 cases may be tabulated as follows. They have been abstracted from the " descriptive rolls " or from information supplied on subsequent inquiries at the instance of the Commission. The Commission cannot, however, vouch for the accuracy of these returns. In one instance an insane of the lower classes, described as a " 2amindar," proved to be a school-boy, the son of a muharir in a munsiff's court.
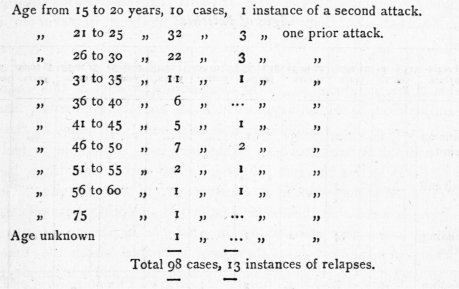
529. The following table shows the relative liability to insanity at different ages, and ages in the hemp drugs cases. This information has been compiled solely from the" descriptive rolls," and in very many instances thea ges entered are doubtless only rough guesses. At all times it is difficult to ascertain the true age of a native of the lower classes, and in the case of wandering insanes, beggars, etc., the determination must necessarily be inexact and a mere approximation :-
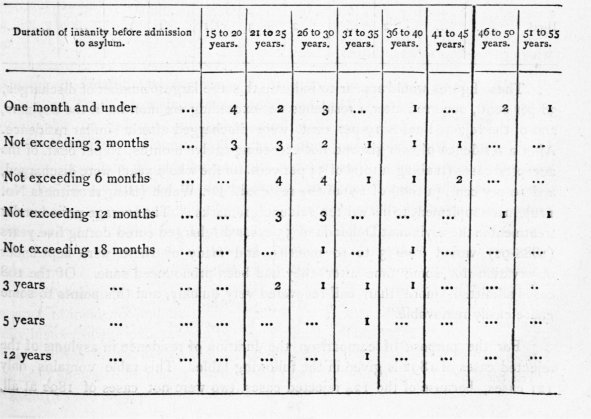
530-. The data for ascertaining the duration of insanity are either unreliable or not procurable in all cases for the periods during which the insanes were at large, and it is only with the duration of residence in asylums that the Commission can give any accurate details. The duration of the insanity before admission into the asylum for the 53 cases for which information is recorded is shown in the following table :—
Out of the 98 accepted cases, 10 were not insane on admission into asylums, 29 were not cured, and 9 died during residence. Regarding the cases described as " not cured," it is necessary to explain that the expression is to be taken only relatively for the period during which the patients were under observation by the Commission, and which as a general rule would be under two years. The duration of residence in asylums of the so patients discharged during the period mentioned may be tabulated as follows :—
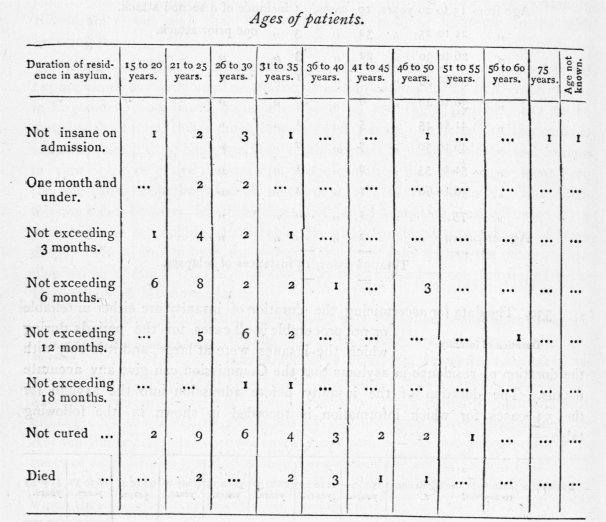
These figures would appear to indicate that the largest number of discharges, 38 per cent., occurred after a residence not exceeding six months in the asylums, and of the rejected cases IQ per cent. were discharged after a similar residence. After a residence of over six and not exceeding twelve months, 16 per cent, of the accepted cases (making a total of 54 per cent. for the whole year) were discharged, and 10 per cent. (a total of 29) of the rejected. Dr. Walsh (Bengal witness No. 112), in a supplement to his written evidence, remarks : " The average period under treatment in the asylum at Dullunda of 55 cases discharged cured during five years (1888-92) varied from 3 to 1 o months, and many of these were kept under observation for some time after they had been pronounced sane. Of the 108 cases admitted, more than half recovered very quickly, and this points to some cause easily removable."
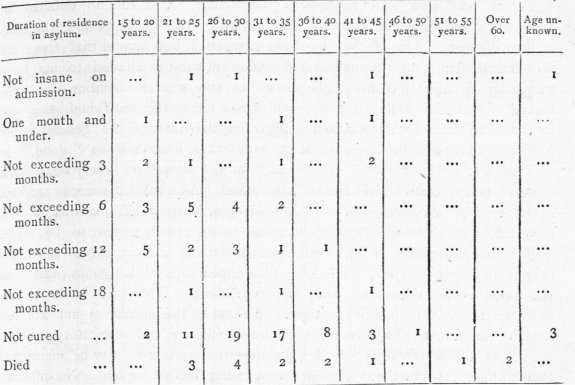
For the purpose of comparison, the duration of residence in asylums of the rejected cases of 1892 is given in the following table. This table contains only 121 cases, because of the 124 rejected cases, two were not cases of 1892 at all, and one was rejected because it has been entered a second time on the statement :—
531. The proportion of recoveries calculated on the 98 accepted cases would amount to 6r2 per cent., or, deducting from both sides the i o patients ,who were not insane on admission, to 56'8 per cent. Calculated in the same manner, the percentage of recoveries of the rejected cases would be 34.7 and 32.4.
532. Calculated on the accepted cases, the mortality amounted to 9.1 percent. In no single case, however, was the death due directly to the mental condition. The mortality in the rejected cases amounted to 12.3 per cent. on the total admissions. There is one fact which vitiates the figures in connection with mortality in asylums.— that is, the practice which exists at all events in the Tezpur Asylum, Assam, of transferring dying patients to the " Moribund Ward " of the Charitable Dispensary for medical treatment.
533. The Commission would premise the analysis of the symptoms presented by the accepted cases by remarking that the information available is extremely meagre. As a rule the asylum records fail to afford a full clinical history of the condition of the patients on first admission, and the subsequent entries in the asylum case books are also frequently lacking in useful information. In one asylum no case book appeared to have been kept up in 1892, The medical certificates on which the patients are admitted into the asylums usually contain only sufficient evidence of the mental state to support an opinion as to the mere fact of insanity. The descriptive rolls are the only source in the vast majority of cases from which the mode of incidence and duration of attack, the habits, and the personal and family history of the patients can be ascertained. The value to be placed on certain entries in the descriptive roll has already been fully discussed. They have been shown to be untrustworthy, and there is no reason to suppose that other entries are more accurate or reliable. In 17 out of 98 cases only is information recorded as to the nature of the onset of the symptoms ; in eight it may be described " sudden ; " in six as " gradual " or " slow "; and in three as " insidious." As a rule no detailed information is ascertainable regarding the nature of the premonitory symptoms or their duration. " Headache" has been mentioned, but beyond that there are no clinical symptoms. Sometimes alteration in habit is alluded to, but more frequently attention has first been drawn to the mental condition by some insane, violent, or destructive act which has led to the individual being sent to a medical officer for observation. Regarding the state of the general bodily health on admission into asylums, in 35 cases it is described as " good, " in zo " fair," in 8 " indifferent, " in 6 " bad, " in 3 " weak " or " very weak, "and in the remaining cases no information is recorded. As a rule no records are kept of the form or measurements of the head, general physical features are not recorded, and thermometrical observations do not usually appear to be made. The facial expression is as a rule not described, and in three instances only is it referred to as " vacant. " The appearance of a " ganja wart " on the palm is mentioned by one Superintendent. The gait is as a rule not described. Abnormalities or signs of disease of the sexual organs are not usually mentioned. The condition of the circulatory and respiratory systems are not as a rule recorded. Under the digestive system it may be mentioned that in fifteen cases food was refused, necessitating forcible feeding. No information as a rule is available regarding the glandular system, state of the skin, or character of the urine. Under the muscular system " tremor " has been referred to and " muscular twitchings like chorea. " But such features as power of "grasp " of hands or reaction to electric stimulus are not mentioned. Under the nervous system—sight, hearing, taste, and smell—no systematic observations appear to be recorded ; in only one asylum was there any record regarding the state of the pupils ; in one asylum redness of the conjunctiva was mentioned ; and in one asylum the eyes are described as " red. " The conditions of nervous sensibility, hyperaesthesia and anaesthesia, do not appear to have received attention ; and in one asylum only are reflex phenomena mentioned.
Regarding mental symptoms. In fifty-six cases incoherence of language is mentioned, in seven uncommunicativeness, in seven silentness, in nine talkativeness, in twelve muttering, and in twenty-two abusiveness or obscenity of language; in four cases the patients were " excited," in three roaring, in twenty-four noisy, in twelve restless, and in thirty-one sleepless. In seven cases there were symptoms of " exaltation," in thirteen quarrelsomeness, in twenty-nine destructiveness, twenty-five were homicidal, twelve suicidal—frequently the same case exhibited both tendencies—and thirty-six violent. In twelve cases there was laughter, in two dancing, in one absurd postures, and fourteen were either sad, crying, or moaning. Forty-six were dirty or filthy in their habits, twenty-one were indecent, in twenty-four there were delusions, and in four cases the patients are described as " childish. "
The alteration in symptoms in the asylum was in some cases very rapid, so rapid in some instances as to be almost immediate. In others the progress towards sanity was slower ; in some there were relapses, with occasional outbursts of violence) while others from being violent and abusive became melancholic or quiet and silly, or drifted into a condition of dementia.
534 The cause of death in the nine fatal cases was as follows : One general debility, one cholera, two dysentery, one leprosy, one heart disease, one diarrhcea, one dropsy and old age, and one no cause assigned. In five of these cases no post-mortem examination appears to have been made ; in the four in which it was conducted, the condition of the brain is not specially noted in three, while in one case—death from cholera—the following note is made : " Weight 43 oz.; both membranes and substance of brain congested, and lateral ventricles contained a very small quantity of fluid. Brain substance firm." As to the results of post mortem examinations in alleged ganja cases, therefore, the evidence is purely negative as to any even coarse brain changes being present. It may be remarked, however, that as a rule when autopsies have been conducted in asylums, it has been solely with the object of ascertaining the cause of death and not for purposes of pathological research. In most cases the brain does not appear to have been examined, and, when it has been examined, the information recorded is so meagre and superficial as to be valueless.
535. Reviewing the mode of incidence so far as it can he ascertained, the type, general symptoms, and duration of cases in which the mental balance has been alleged to have been overthrown by the use of hemp drugs, the question arises are there any symptoms pathognomonic of the condition generally known as hemp drug insanity, and on what does the evidence rest that the use of these drugs may induce mental aberration ? The evidence obtained by the Commission appears to indicate that in the cases of alleged hemp drug insanity which find their way into asylums, there are no typical features in the premonitory symptoms and no pathognomonic symptoms in the insane condition on which to base a determination of causation. The mode of incidence, the premonitory symptoms, and the symptoms of the insane state are practically the same in cases in which these drugs have never been used as in instances in which the mental equipoise has been accepted as being disturbed by their employment. The type of hemp drug insanity is mania, though in the subsequent history of a few cases there appears to be divergence from the type. The mania may be acute or chronic. The majority of medical witnesses who have studied the subject are clearly of opinion .that there is nothing typical in the symptomatology of hemp drug mania to distinguish it from mania due to other causes. But at the same time several express an opinion that the symptoms are of shorter duration in hemp drug mania than in mania due to other causes. Besides this pretty generally accepted view that short duration is a diagnostic mark of hemp drug insanity, one or.two witnesses are inclined to think that there are other characteristic symptoms. Dr. Cobb (Bengal witness No. I to) in his oral evidence states : " There is nothing very typical in the symptoms, but still ganja insanity has points of distinction from other kinds of insanity. It is very temporary. Confinement of the patient with removal of the exciting cause generally brings about rapid cure. Delirium is a prominent feature. There are other general features which it is difficult to put into words, and which experience alone can teach ...One recognizes ganja insanity intuitively. All the symptoms I have described may be present in other kinds of insanity, but one judges by the combination of them." Dr. Crombie (Bengal witness No. 104) in the appendix to his written evidence states : " I refer to the peculiar characters of this form of toxic insanity by which it can be recognized just, or nearly as readily, as those of delirium tremens distinguish alcoholic intoxication. To enable me to do so clearly, it is necessary to distinguish between acute ganja intoxication due to a single debauch or to continuous excessive use of it in what might be called a bout of ganja drunkenness, and the effects of its continued immoderate use over a lengthened period of time. Acute ganja intoxication is marked by the extreme vehemence of the mania. In its mental, moral, and muscular manifestations, it bears no resemblance to alcoholic intoxication whatever. The maniac is excited in every fibre. .His aspect is infuriated, his eye glares and is tense and glistening, while at the same time the conjunctiva is red and injected. He shouts, vociferates, sings, walks quickly up and down or round his cell, and shakes the door out of its fastenings. If at liberty, he is violent and aggressive, and may run amok. In other cases the mental disturbance is less marked, but the demeanour is excited, and he suddenly seizes some weapon, and slays one or more of the people in his neighbourhood without apparent reason. The attack is of short duration, being limited to a few days. Then there is perfect recovery, and the patient is oblivious of things which took place during the period of intoxication... The insanity produced by the long-continued immoderate use of ganja has also features of its own. The patients are hilarious, attitudinise, and are full of the sense of wellbeing ; they are as a rule good-natured and trustworthy, and recover in a large proportion of cases under confinement and deprivation of the drug. These cases characterize Indian asylums by the large number of happy amusing lunatics they contain. They are, however, very subject to relapses even after lengthened periods of freedom from symptoms."
The alleged shorter duration of hemp drug cases is to some extent borne out by the statistics obtained by comparing the accepted and rejected cases for 1892. In the accepted cases (98), after deducting the ten patients who were not insane on admission, the percentage of recoveries has amounted to 56.8 per cent. of the total admissions, while of the rejected cases only 32.4 per cent. of the admissions have recovered. The Commission consider, however, that too much stress should not be placed upon rapidity of recovery as a diagnostic sign in attempting to differentiate between hemp drug and ordinary mania. It is well recognized that as a rule ordinary uncomplicated cases of mania rapidly recover. Moreover, bearing in mind that hitherto hemp drug cases have been accepted as such as a rule on untrustworthy evidence, and that consequently many of the cases on which Superintendents of Asylums have based an opinion as to the relative rapidity of cure of hemp drug and ordinary mania were not actually toxic cases, "rapidity of recovery " can only be accepted tentatively as a means of discrimination. It is scarcely necessary to observe that this so called " diagnostic mark" has not been used in diagnosing hemp drug insanity in the asylums, as it has been shown that diagnosis was made on the admission of the patient and not after his recovery.
In connection with the alleged greater recoverability of cases of hemp drug mania, it may be of interest to quote statistics of cases in an English asylum. In the West Riding Asylum the percentage of recoveries in acute and simple mania were respectively 65.5 and 61 per cent., while 8.4 and 11.9 per cent. were relieved and 11.9 and 16 per cent. formed a chronic residue. Taking all maniacal forms in the same asylum (including the simple, acute, hysteric, chronic, delusional, recurrent, and puerperal), the recoveries amounted to 53.2 per cent. : 14 per cent. were relieved, and 2cr6 per cent. formed a chronic remainder. Obvi. ously, however, these figures are not strictly comparable with the statistics of the hemp drugs and rejected cases with which the Commission have been dealing, because the Indian cases have only been a limited period under observation—under two years—while the West Riding Asylum statistics refer to periods of several years.
In considering the " peculiar characters " of hemp drug insanity as alluded to by Dr. Crombie, the Commission have to recall. attention to the erroneous character of the statistics which form the basis of that officer's conclusions, and also to point out that generally all the features of the acute form as described by Dr. Crombie are comparable with the symptoms of transitory mania and the symptoms of the chronic form with those usually found in cases of mania unconnected with the use of hemp drugs. Indeed, Otto Von Schwatzer's description of transitory mania in the Dictionary of Psychological Medicine might be read in lieu of Dr. Crombie's " peculiar character " of the symptoms. " The principal characteristic of transitory mania is the spontaneous and ungovernable intense excitement produced by the cerebral irritation and the morbidly 'exaggerated motor impulse, which, however, does not consist, as in other and milder forms of frenzy, of a more or less harmless restlessness, but in a wild paroxysm with a blind desire of destruction. The excitement extends with great intensity over the whole of the motor sphere, so that not single muscles, but the whole muscular system, is under its influence. All the wild motor discharges are without any purpose and object Every idea is at once expressed either by words or by inarticulate cries, screams, and shouts...............lively and sparkling eyes, which protrude from the orbits, redness of the conjunctiva, threatening or staring look As rapidly and suddenly as the attack comes, so suddenly it also disappears. Another abnormality of transitory mania is that its duration•may be very much protracted, there being cases in which the attack lasted several days ... Recollection generally reaches as far as the moment of outbreak, and perhaps includes darkness before the eyes, etc., but then completely ceases." The description of some of the symptoms usually found in cases of mania, as given by W. Bevan Lewis, is also fairly comparable with Dr. Crombie's account of the special features presented by cases of insanity produced by the long-continued immoderate use of ganja. " The excitant swell of feeling and the torrent of disconnected ideas may express themselves in continuous garrulity, in noisy chattering, in threatening and abusive tones, in laughter, in singing, or loud shouting with corresponding pantomime and almost ceaseless activity, or the feeling of unusual freedom and energy may find relief in destructive tendencies, smashing of glass, breaking of furniture, tearing of clothing, or, perhaps, in violent aggressiveness." In regard to these lunatics being " very subject to relapses," it may be remarked that this also is recognized as a common feature in ordinary cases of mania.
536. Summing up the evidence as to the presence of pathognomonic symptoms in cases of hemp drug insanity, the Commission consider that, with the exception perhaps of the shorter duration of such cases when compared with cases of ordinary mania, there are no symptoms by which the cause of the mental condition can be determined.
The determination of cause depends wholly upon history. The Commission also consider it not improbable that there are no typical brain lesions peculiar to hemp drug insanity, though definite lesions are doubtless present in chronic cases, as they are in cases due to other causes.
In answering the question, therefore, on what the evidence rests that hemp drugs may induce mental aberration, the Commission would offer the following remarks : The evidence may be considered under two heads—(a) popular ; (b) scientific. The popular idea that the use of hemp drugs may induce insanity can be traced back for many. centuries, and the present day views on the subject are no doubt the outcome of old popular ideas which have been handed down and become concrete. With non-medical witnesses the mere use of the drug along with the fact of insanity, as the evidence shows, has as a rule been accepted a% cause and effect. Of the large number of medical witnesses who have given evidence before the Commission, probably not a single one has ever observed the inception of the habit and the use giving rise to mental aberration, and been in a position to gauge the value of other contributory causes if present. With practically no modern literature on the subject, with no special knowledge apart from the popular idea, with a very slight or no clinical experience of insanity in England, with the experience derived from perhaps having had half a dozen insanes in the course of two years under observation as Civil Surgeons, officers have been placed in charge of asylums, and have had to differentiate between cases of hemp drug insanity and ordinary mania. The careful inquiry which has been made by the Commission into all the alleged hemp drugs cases admitted in one year into asylums in British India demonstrates conclusively that the usual mode of differentiating between hemp drug insanity and ordinary mania was in the highest degree uncertain, and therefore fallacious. Even after the inquiry which has been conducted, it cannot be denied that in some of the cases at least the connection between hemp drugs and insanity has not been conclusively established. But taking these accepted cases as a whore, we have a number of instances where the hemp drug habit has been so established in relation to the insanity that, admitting (as we must admit) that hemp drugs as intoxicants cause more or less of cerebral stimulation, it may be accepted as reasonably proved, in the absence of evidence of other cause, that hemp drugs do cause insanity.'
The action of hemp resin, the active principle of all forms of the drug, when taken internally, has formed the subject of accurate experimental observations, and the physiological action of the drug on the human subject and animals is fairly well known. When, however, the products of the destructive distillation of the resin are inhaled, as in ganja smoking, the precise physiological effects induced have not hitherto been, so far as the Commission are aware, as fully studied. Dr. Russell's experiments (Bengal witness No. to5) already quoted are, the Commission understand, the only ones instituted on man with any pretensions to scientific accuracy. On the other hand, Assistant Surgeon Bocarro (Sind witness No. 20) and others refer from careful actual observations to the general physiological effects induced by smoking ganja and charas. With the object of elucidating the physiological effects of the products of the destructive distillation of hemp resin, Dr. D. D. Cunningham, F.R.S., Professor of Physiology, Medical College, Calcutta, at the request of the Commission, kindly undertook a series of experiments on monkeys. A full account of the experiment with ganja is given in paragraph 483. Dr. Cunningham reports on naked-eye inspection that " the cerebro-spinal nervous centres were all apparently perfectly healthy." The results of the histological examination are not before the Commission, but it is hoped that they will be received in time to be included in the appendix. So, far as the information from all sources before the Commission is concerned, there is no evidence of any brain lesions being directly caused by hemp• drugs, as they have been found to be caused by alcohol and dhatura ; and there is evidence that the coarse brain lesions produced by alcohol and dhatura are not produced by hemp drugs.
537 The precise physiological effects induced by the inhalation of the products of the destructive distillation of hemp resin and those arising from the exhibition of the resin by the stomach are probably not identical, but in both cases there is ample evidence that the use of the drug in either form may first cause cerebral stimulation, and then depress the functional activity of the brain. Francois Franck and Pitre's experiments (Arch. de Physiol., 1883), quoted by Lauder Brunton, indicate that in the case of dogs the excitability of the brain is increased by the administration of Cannabis, a purified form of hemp resin, so that the tendency to epileptic convulsions is greatly increased, and may be induced by very much slighter stimuli than usual. Alcohol is a typical cerebral stimulant, and any drug which, like alcohol, increases the functional activity of the brain, may, like alcohol, give rise to what is technically known as " an intoxication." The effect of alcohol may result in three principal sets of symptoms, which are admirably se tforth by Legrain (Dictionary of Psychological Medicine).
(a) Taken in large amounts, in a short time it produces acute symptoms, which are immediate, but temporary—intoxication or drunkenness.
(b) Alcohol if taken often and in great quantities, or if the drunkenness is nearly continuous, or if the individuals are not very strong in brain, accumulates in the organism without being at any time completely eliminated, and gives rise to acute symptoms of longer duration than mere intoxication—delirium tremens.
(c) Alcohol regularly or irregularly introduced into the system for a long time in doses even shOrt of producing immediate symptoms is known to produce general disorders and progressive lesions, characterized by weakening of the faculties and premature dementia, the ensemble of the symptoms constituting chronic alcoholism.
The analogues of these chief effects of alcohol may also be traced in the symptoms induced by hemp drugs, in which we have—
(a) The condition of more or less delirium with hallucinations and merriment as occurring in a person who has taken what is to him a large dose of the drug, the symptoms being only temporary—hemp drug intoxication.
(b) The condition of wild frenzy, with symptoms of transitory mania occurring in a person who has systematically indulged largely in the drugs—hemp drug delirium.
(c) Cases in which the drug has been used for a considerable period, and then given rise to mania of shorter or longer duration, or cases in which the symptoms of hemp drug delirium do not completely subside, but pass on into a state of mania usually curable, and thus indicating the probable absence of anatomical lesions—hemp drug mania.
The evidence, though by no means clear and decisive, is perhaps sufficient to justify the presumption of an analogy such as is above indicated ; and cases which have come before the Commission have seemed to divide themselves into these three classes. At the same time it must be pointed out that the sharp line of demarcation in symptoms which separates alcoholic intoxication from delirium tremens does not separate the intoxication and delirium produced by hemp drugs. Further, in regard to what has been said about hemp drug mania, it may be noted that it is not improbable, though it has not been established by evidence, that prolonged abuse of the drugs may give rise in some cases to definite brain lesions resulting in a progressive weakening of all the faculties leading to dementia.
538. Hemp drugs have been classed among the " poisons of the mind," and it may be of interest, as throwing a good deal of light on the whole subject and explaining the different modes in which " intoxications " may give rise to altered mental states, to allude briefly to the manner in which mental poisons are presumed to act. M. Legrain, in Hack Tuke's Dictionary of Psychological Medicine, defines mental poisons as including all substances, whatever may be their origin and nature, which are capable of exercising a marked action on the intellectual processes, either by disordering them or by suspending them completely for a moment or longer. Ne then goes on to describe their action at length in a passage which may be summarized as follows. Poisons of the mind act primarily to a greater or less extent,on the cerebral cells. Almost all substances introduced into the organism modify the cerebral processes, this being due to the delicacy of the organization of the nervous system, which, like all complicated mechanism, is extremely vulnerable. The brain as the terminus of all sensations, and as the regulator of even the most minute cellular functions, has to bear the brunt of attacks, even the slightest, directed against the vital equilibrium, and has also to re-act in order to re-establish this equilibrium. In every intoxication, in addition to the cerebral re-action due to the effect of the poison itself, there are other re-actions requiring as many reflexes for the defence of the body, and closely connected with the impressions which the sensorium receives, of modifications of nutrition, or of changes which take place in other organs under the influence of the poison. These reactions are the symptoms common to every intoxication. The cerebral re-actions which take place under the more direct influence of the toxic substance are of two kinds—they may be diffused, general, and undefined, and expressed by vague symptoms, indicating a lesion of the brain as a whole ; or they are well-defined, clear, and localized, indicating that the poison affects one special centre of the brain to the exclusion of all others. Special derangements may also occur in addition to those of the brain. In spite of the great dissimilarity of the substances which are capable of producing cerebral intoxication, there are nevertheless certain clinical features common to all. We might even say that there are no intellectual disorders more pathognomonic of one poison than of another. The artificial insanity produced by toxic substances is nothing but the re-action of the cerebrum, which is arrested in its full and regular function, and the coming into play of the cellular elements under the influence of an external and abnormal excitation which is different from the usual stimulation. As already pointed out, this excitation may affect one part of the brain more than another ; hence the apparent difference in the symptoms, which may also vary in different individuals, although they are under the influence of the same poison. The toxic substance does not add any new element to those which the normal brain possesses, and herein lies the great difference between the superadded insanity and the insanity which the brain produces itself between toxic derangement and psychosis. All or nearly all slight intoxications, from whatever cause, are characterised by certain general symptoms—(I) excitation of the organ of thought ; (2) intoxication ; and (3) incoherence of ideas and actions. In organic derangement there is a qualitative ideational alteration ; in toxic derangement there is only a functional disturbance, and a quantitative modification of psychical expression. The special symptoms are of infinite variety, and this variation of the special phenomena depends upon two factors — (a) the localization of the toxic effects in a special cell group in the brain ; and (b) on individual re-action. Nervous and predisposed persons appear to be more easily affected than normal subjects. Certain toxic substances, such as alcohol and morphia, etc., do not produce the same effects on all individuals, male or female, under all latitudes. A large number of substances produce cerebral effects, but rarely in consequence of certain individual dispositions. Among labourers who handle carbon disulphide or aniline, some only present mental disorders. The individual factor with its idiosyncrasies plays here, as everywhere, a very important part. There are other factors, too, which have to be considered, the degree of education, reason, locality, dosage, and mode of preparation of the drug, all of which may modify the symptoms. Thus the hallucinations of the Western people under the influence of hashish are not identical with the voluptuous dreams of the Orientals. The simple intellectual disorders produced by various poisons are of two kinds—( I) the condition of excitement, and (2) the condition of depression ; but these two conditions do not exclude each other. Thus in the case of hemp drugs, depression or narcosis usually follows the initial excitement. In addition to the intoxication and general disturbance of the mind, mental poisons produce also insane conditions or mental disorder. But these conditions are intimately connected with the general disturbance of the mind. The individual variations are here very numerous, the same poison producing different effects in two individuals. The insane conditions have been classed into several groups—( 1) maniacal or incoherent type is the most frequent, the derangement being absolutely general ; (2) alcoholic type, a maniacal condition of a depressive, painful, and frightful form ; (3) maniacal type of expansive form, ambitious, mystic, and erotic ideas, idea of self-satisfaction and of exaggeration of personality—this form is considered as representative of hashish, etc. ; (4). melancholic type ; (5) mixed forms in which depression may alternate with excitement ; and (6) vesani conditions, i.e., attacks of insanity, which, although excited by poisons, do not derive their special colour or character from the drug, but arise in persons strongly predisposed to insanity. Most poisons produce nothing but temporary disorders, which disappear without leaving any trace behind : their effect is limited to a slight excitement on depression of the faculties, to a short intoxication, or to a more or less profound narcosis ; afterwards perfect order is reestablished. Other poisons cause more serious symptoms. The duration of symptoms varies according to the individual disposition and the dose absorbed ; but, generally speaking, the acute stage, if recovery should follow, does not last more than a few days or weeks. In chronic voluntary intoxication the cause of the symptoms depends necessarily on the habits of the patient and the individual re-action. The chronic period does not generally establish itself from the first. There are first the acute phenomena, which may reproduce themselves a number of times, without, however, preventing chronicity from establishing itself : these acute symptoms are nothing but epiphenomena, which appear again and again in the course of this period : the two essential kinds of symptoms, however, are the irresistible appetite for the poison, with periodical return of the acute and sub-acute symptoms, and the progressive decay of the mental faculties. The acute symptoms correspond to the temporary saturation of the body with the poison, while the chronic symptoms are the expression of definite anatomical lesions in the brain gradually developed under toxic influence. The prolonged use of mind poisons thus gives rise to progressive weakening of all the faculties passing over into dementia. Acute toxic insanity is a secondary insanity : it is polymorphous ; all forms of insanity may be observed, not only in two different intoxications, but even in the course of one and the same intoxication. It is temporary, nothing but a momentary acute effervescence terminating with the elimination of the poison.
539. Before leaving the subject of insanity, there is one point to which it seems desirable briefly to allude.. The impression left on the minds of the Commission by the perusal of a large number of records in criminal cases and by the examination of some asylum cases is that there is occasionally seen a tendency to confound intoxication and insanity in connection with hemp drugs. The result is that in some cases men who should have been simply punished for being intoxicated have been sent to the asylum, and, though sane when they reached that institution, have been detained there. These cases are, however, much rarer than they used to be, if one may judge from the old asylum reports. A more serious result of this confusion is that there are cases in which men who have committed offences, especially crimes of violence, under the influence of hemp drugs have been acquitted on the ground of insanity, although the circumstances have been such that had the intoxicant been alcohol, they would have been convicted. It is undoubtedly more difficult in the case of ganja than in the case of alcohol to recognize the line drawn for social and legal purposes between intoxication and insanity. But the difficulty is not insuperable. The main reason for the confusion that has existed is probably the ignorance that has prevailed regarding hemp drugs. When they are recognised as a common intoxicant, it is to be hoped that the practice of the Courts will be freed from the occasional blemishes above indicated. It is not expedient, nor is it just, that intoxication from hemp drugs should secure immunity from punishment which is not allowed to alcohol ; and, on the other hand, the Commission cannot concur with Dr. Walsh (Bengal witness No. 112) when he says : " It is not my opinion from experience that it is either dreadful in itself or possibly disastrous to a man's mind to have to herd for years with lunatics, though sane."